
An ongoing dialogue on HIV/AIDS, infectious diseases,
November 3rd, 2019
Learning the Names of HIV Drugs Is Horribly Difficult — Here’s Why
Happens every time. We start teaching about HIV, and at first, everything is going great.
Epidemiology, pathogenesis, diagnosis, clinical presentation. The students are right there with us.
However, then we start covering treatment — and things immediately get tricky.
Because no matter how engaged and brilliant they are, and no matter how scintillating we are, when the long list of antiretroviral agents appears, their eyes glaze over with fatigue.
Instant somnolence. Like someone turned up the temperature in the room, dimmed the lights, and passed out soft blankets and pillows.
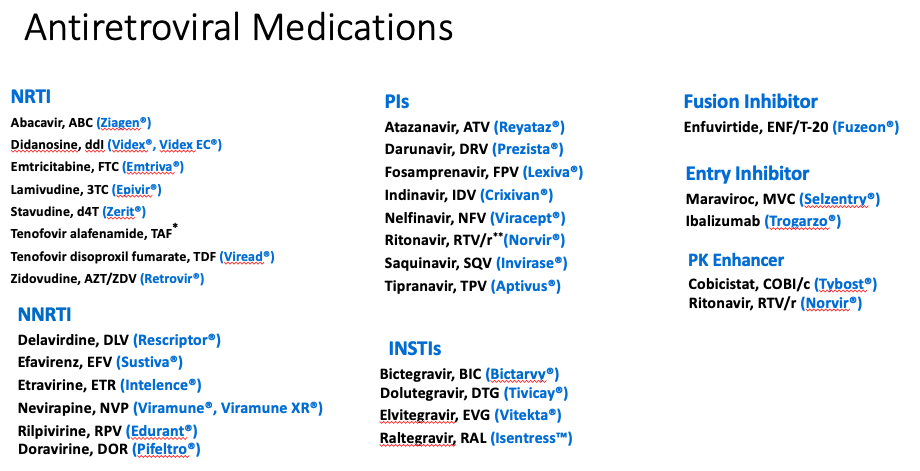
And it’s no wonder! There are lots of drugs, with a dizzying array of names, abbreviations, combination tablets, and mechanisms of action.
We haven’t helped matters by following these RULES OF HIV MEDICINE, all of which were designed by evil creatures (with advanced degrees in medicinal chemistry and marketing) to make learning HIV medications terrifying. Here are these baleful rules:
- All drugs must have at least three names. Generic, brand, and 3-character abbreviation. To make matters worse, some have more than three names, starting with the very first drug way back in 1987, zidovudine. It was also called AZT (that’s what most people called it), ZDV, and Retrovir (that’s 4, including zidovudine). It also showed up in Combivir and Trizivir, for good measure. Now that’s just mean.
- HIV specialists must refer to them by different names at different times, for no apparent reason. Do we do this to maintain our special status? To be whimsical? To deliberately confuse others, just for sport? Whatever the motivation, it’s working wonderfully to keep this knowledge the very definition of arcane.
- Names of combination tablets should have nothing in common with their parent drugs. Some recent examples: Combine Tivicay and Epzicom — what do you get? Triumeq, of course. Descovy plus Edurant? Odefsey! See, isn’t this fun?
- Some of the abbreviations must bear no resemblance to either the generic or the brand name. Example — what does “3TC” have to do with the word “lamivudine,” for which it is the widely accepted abbreviation? Hint: nothing. Unless you check its chemical structure. And who, we might ask, will be doing that? And since emtricitabine is very similar to lamivudine (you knew that, right?), emtricitabine is abbreviated “FTC,” which makes all kinds of sense since emtricitabine starts with an “F.” (Oh wait. No it doesn’t.) The first time this disconnect between the true and abbreviated name came up was with the abbreviation for the drug zalcitabine, which was abbreviated “ddC”, for a chemical name that no one used. That’s right, two small “d”s followed by a capital “C.” Careful readers will note that zalcitabine has neither a single “d” nor a capital “C.” Fortunately, few prescribed this lousy drug anyway, which made its suitably horrific brand name (“Hivid”) just a faint stain on the history of HIV drug development.
- Names of different drugs might sound alike, but will have nothing whatsoever to do with each other. Nelfinavir (Viracept) and nevirapine (Viramune) give us an example where both the generic and the brand names sound kind of similar. But they are completely different drugs — different dose, mechanisms of action, side effects. About the only thing they have in common was that they are both HIV treatments. You think people have confused them? You bet.
- Drugs should change their names when they come out in different formulations. Take a look at the various name changes when tenofovir disoproxil fumarate (TDF) spawned tenofovir alafenamide (TAF) — this generated a whole new crop of confusing drug names, as both are extensively coformulated. But the trickiest (and saddest) story is saquinavir, the very first protease inhibitor. First it was Invirase, taken as three 200 mg capsules three times a day. Due to poor bioavailability, Invirase was later changed to the humongous soft-gel capsules called Fortovase, taken as six capsules three times a day. (Yes, that was the dose — it was practically a patient’s whole diet.) Then, with the realization that humans could not subsist on a drug that was six large capsules three times a day, saquinavir went back to being Invirase, but now had a new size (500 mg), and was taken as two tablets twice daily with ritonavir twice daily. Got that? Of course not.
- The order in which drugs are listed in combination pills will be different in different sources. After years of litereally everyone writing TDF/FTC as the abbreviation for the pill that contains tenofovir disoproxil fumarate (TDF) and emtricitabine (FTC), along comes the first PrEP study, which reversed them. Not only that, they used a dash rather than a slash — “FTC-TDF.” Because why? And with three- and four-drug combinations, which drugs goes first? What’s the order? Alphabetical? By mechanism? Your guess is as good as mine.
- If people are getting used to the three-letter abbreviations, go ahead and abbreviate the drugs in combination tablets with one letter, not three. This is a relatively recent trend, but one that people eager to make HIV drugs harder to learn surely must support. Example: When darunavir is given with ritonavir, it’s often written “DRV/r.” Ritonavir is changed to a lower case “r” (and not abbreviated RTV) to denote that it is not being used as an antiviral, but as a pharmacokinetic booster. Makes sense, sort of, except that nobody shared the code. However, the slash implies that it’s a combination tablet, which it most certainly isn’t. When we write or say “DRV/c,” or Prezcobix, however, this is a combination tablet, with the “c” standing for “cobicistat.” So cobicistat is also abbreviated as one letter, unless you are fans of the cute-sounding “COBI,” which is four letters, and for the record is pronounced like the former Los Angeles basketball star and the famous Japanese beef, but definitely has nothing to do with either one of them. But why stop there and let darunavir have all the fun? Let’s move right on to “ECF-TAF,” which stands for elvitegravir, cobicistat, emtricitabine (FTC, remember?), and tenofovir alafenamide (TAF). Certainly it makes all kinds of sense to use single letters for three of the four drugs in this combination tablet, then three letters for one of them — following a dash. Right? I mean come on, it’s so obvious.
So what’s a poor clinician to do? Some great responses here, I especially liked this one:
I’ve had folks threaten to get an interpreter when we were discussing HIV meds in our hospital formulary meeting.
— Adam Lake MD (@ACLakeMD) November 3, 2019
My solution (ha) to this mess will come in Part 2 of this topic. In the meantime, I welcome your input about how we should go about teaching (or learning) this material.
And it’s obviously time to reprise this classic. Take it away, Trip!
17 Responses to “Learning the Names of HIV Drugs Is Horribly Difficult — Here’s Why”

Paul E. Sax, MD
Contributing Editor
NEJM Journal Watch
Infectious Diseases
Biography | Disclosures | Summaries
Learn more about HIV and ID Observations.
 NEJM Journal Watch — Recent Infectious Disease Articles
NEJM Journal Watch — Recent Infectious Disease Articles- RSV Infection Substantially Raises Risk for Cardiovascular Events
- Pediatric Hospitalizations for Mycoplasma pneumoniae Rose Sharply in 2024
- Sulopenem, a New Antibiotic for Uncomplicated Urinary Tract Infection
- Is Cardiovascular Risk Sustained After SARS-CoV-2 Infection?
- Which Hepatitis B Vaccine Provides the Longest-Lasting Protection in People with HIV?
It’s easy for us old-timers, who learned the drugs and their crazy names as they became available. But for everyone else it must be like reading a Russian novel. (In “Dr. Zhivago,’ the main charter was referred to as Yuri, Yura, Yurochka, Yuri Andreyevich and Zhivago. And that was easy compared to Tolstoy!)
There’s yet another point of confusion. There are a number of HIV educators out there who either can’t remember the 3-letter abbreviation, don’t agree with the choice, or just don’t care, so they just make up their own. DRV becomes DAR, RAL becomes RGV, and EVG becomes ELV. This does NOT help!
I suggest that, for the purpose of report and communication, to use only the generic names with 3 letter abreviton. The generic names make some sense relative to drug class. The brand names only add confusion.
For those not swimming in the alphabet soup each day, I just tell them to learn 3-5 STRs (another TLA for you (why no reference to TLA (Three Letter Acronym?))). Problem is there are now more than 10, and with generics going live, we’ll see more – Symfi-Lo I’m looking at you…
There is no reason for med students to remember names of specific HIV drugs (nor for medical residents etc). I expect my students to remember the drug classes and maybe only few important specific drugs
Oh and what about SDF (? Single daily formulations) basically means one tablet dosing. TLE? TLD?
The Tower of Babel has won. The names are gibberish and non-descriptive. Soul-less ones are even trifling with “3-letter words”. Possible benefits of rhyming final syllables include further musical whimsey, perhaps recasting antiviral drugs in a Gilbert-and-Sullivan style lampoon, or a la Tom Lehrer’s treatment of “The Elements”.
Since we appear to be saddled with nonsense syllables mined from the pull of a Los Vegas-style 1-armed bandit, my personal preference would be to retain instead a board-certified spirit medium to communicate with the departed Dr. Suess, and assign meaningless BUT DELIGHTFUL names to the drugs. Some of these could spawn their own “3-letter words”, e.g., Foona-Lagoona Baboona becomes FLB. Related drugs could be grouped under fanciful family names……it would be far easier to remember a pedigree such as “Trouble 1” and “Trouble 2”.
I guess like Joel I qualify as an old timer. It was pretty manageable until the naming consultants started to work on the STF (or is it SDF) names. Those names led me to use the 4 letter abbreviation – PITA, and keep my phone handy
Hah! I couldn’t agree more. I’m a pharmacist and medical writer. I’ve been updating HIV drug monographs for over 20 years. Reading the HIV guideline updates is absolute alphabet soup, especially when fixed-dose combos are discussed. I keep an abbreviations list handy because every once in awhile FTC vs. 3TC still gives me brain freeze.
An earlier commenter brought up Symfi vs. Symfi Lo. I’m kind of surprised what we haven’t had drug errors with those two getting switched. BTW, the brand names sound like COCs (combined oral contraceptives).
Well, the simplest solution would be NOT testing students on the medication list, as there is no point to master minutia. The current model of students’ evaluation – rote learning, multiple choice questions – has zero applicability to their future medical career, it’s just easier to construct. You can always tell your students “Don’t bother writing down this long list of names. No such pointless question will count toward your marks in any of my lessons. That is a promise.” (ibid)
In real life, physicians know the medications they’re using through practice and have access to uptodate, micromedex, etc.
https://m.9gag.com/gag/axVAjWp/how-big-pharma-name-their-new-drugs
I thought Oncology was bad. Now there’s something worse!
With EPIC EHMR I have constructed “dot” phrases for all the HIV drugs that include the generic name, the brand name (with a ® symbol alt-0174 if you need to know) and perhaps now I will include an abbreviation as well. It is our JOB as specialists and experts to be very clear with the language and consistent. I would almost say that it is imperative that we do so. I have never found any other specialty that takes this responsibility seriously, especially with the wild proliferation of the “nibs” and the “mab” drugs, whose names both generic and trade, are diabolically designed to obfuscate.
I also have dot phrases for antibiotics and bacterial names – there is no excuse in the electronic age to use short hand, acronyms or abbreviations.
You actually made me laugh out loud. Thank you. It was much needed today. I always thought that being an HIV specialist meant that you HAD to use all three names for a drug in the same sentence. I agree with Joel. It was easier to learn these in little aliquots over time. It must be pretty imposing to have it all dropped on you at once.
So simple. They just should have done the same thing that has been done longs ago for Cephalosporins or Penicillins. I mean first generation antiretroviral agents, second generation … and so on.
I stuck to generic names and it drove my patients nutso–for some it was a short trip.
Two comments:
1) what about the suffix rules used for naming anti-HCV DAA? Why HIV specialists didn’t have that ideia?
2) When Roy Gulick is going to sing his updated serenade?
Using acronyms or difficult terms to render medical language incomprehensible to outsiders is a time-honored tradition in medicine. In the olden days we used Greek and Latin. Now we add all kinds of abbreviated terms especially when we come to molecular medicine. Even with specialists in the same field they may not understand each other. One research worker spent some time trying to find out more about STK11 until he found it was the same molecule as LKB1 that his own colleague was working on all the the time. And the list of CD105, END, ENG, FLJ41744, HHT 1, ORW, ORW 1, all mean the same item. We need a super computer, not human brain, to sort these things out.
Did the second part of this article become available?