
An ongoing dialogue on HIV/AIDS, infectious diseases,
February 5th, 2017
Case Report of PrEP Failure: What Can We Learn From It?
The New England Journal of Medicine has published the first well-documented case of HIV pre-exposure prophylaxis (PrEP) failure despite good medication adherence.
We heard lots of this information at CROI last year, and again I’m impressed at the extraordinary degree of virologic investigation done on a case from clinical practice.
To refresh your memory, here are the critical details from the published case report and the supplementary appendix:
- A 43-year-old man began PrEP with TDF/FTC in April 2013, and had multiple negative 4th generation HIV screening tests over the next 21 months.
- Pharmacy refill records indicated excellent adherence. (Side note to young clinicians: Refill frequency is an amazingly powerful tool to monitor adherence.)
- Prior to diagnosis, he had multiple sexual exposures, including receptive anal intercourse without the use of condoms.
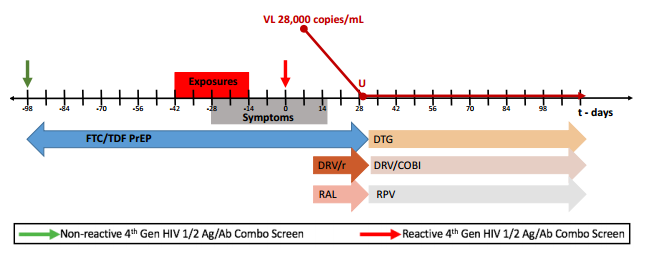
- A couple of weeks before his first positive HIV screening test (antigen positive, antibody negative — Day 0), he developed abdominal pain which waxed and waned over the next 3 weeks. A CT scan demonstrated thickening of the sigmoid colon, ascending colon and rectum. Endoscopy revealed erythematous patches of the sigmoid colon.
- Adherence was confirmed by analysis of a plasma sample obtained on Day 0 revealing tenofovir concentrations consistent with recently taking the drug.
- HIV RNA peaked at 28,000, and became undetectable with the addition of boosted-darunavir and raltegravir.
- His viral isolate had extensive multi-class resistance, including to FTC (M184V), TDF (multiple thymidine-associated mutations), NNRTIs (Y181C), and first-generation integrase inhibitors (92Q).
- He’s now virologically suppressed on DRV/c, RPV, and DTG.
The supplementary appendix has an excellent figure of the timeline, which I’ve pasted below:
So what can we learn from this single case?
- PrEP is very effective, but it’s not 100% protective. I don’t think clinicians are claiming 100% effectiveness, but PrEP-takers may be hearing this from various “experts”, or may be misunderstanding the data.
- Transmitted drug resistance will weaken PrEP. Although all of the mutations in the case are to drugs not in the TDF/FTC combination — except M184V — the multiple TAMs could have weakened TDF through cross resistance. Furthermore, FTC could have been transmitted, or alternatively selected by period of viral replication after viremia developed. The source patient’s virus was not available for sequencing, unfortunately.
- The symptoms of acute HIV infection are highly variable. The supplement to the case reports states, “The patient did not have classic symptoms of acute HIV seroconversion”, which is true — but he did have GI symptoms, which are quite common in acute HIV. We need to remember this variability when following patients on PrEP.
- The monitoring strategy recommended by the CDC in the guidelines should be followed. Although it might seem like overkill to monitor for HIV and other STIs every 3 months while receiving PrEP, remember that only those at highest risk for getting HIV should be receiving PrEP to begin with. Clinicians may choose to recommend more frequent monitoring if clinically warranted.
- Integrase resistance is rare in clinical practice, and transmitted integrase resistance is even less common. While some might interpret this case report to indicate a need for baseline integrase testing for newly diagnosed individuals, the detection of transmitted integrase resistance in most studies of newly diagnosed patients is less than 1%, and often 0%. Notably, the transmitted virus was still sensitive to dolutegravir (I’d interpret the genotype as fully susceptible).
Ok, that’s what I learned. Provides a cautionary note to those both prescribing and receiving PrEP, one further reinforced by this additional case report of PrEP failure presented at a recent conference.
As for tonight’s game, below is what I’m going to watch, and here’s why!
[youtube https://www.youtube.com/watch?v=15SdPnof0FY&w=560&h=315]
23 Responses to “Case Report of PrEP Failure: What Can We Learn From It?”

Paul E. Sax, MD
Contributing Editor
NEJM Journal Watch
Infectious Diseases
Biography | Disclosures | Summaries
Learn more about HIV and ID Observations.
 NEJM Journal Watch — Recent Infectious Disease Articles
NEJM Journal Watch — Recent Infectious Disease Articles- How Well Do Public and Private Healthcare Providers Manage Chlamydia and Gonorrhea?
- Delivery of Malaria Vaccine Through National Immunization Programs: Achievable and Safe
- For Coordinating Management of Opioid Use Disorder and Hepatitis C Infection, Telemedicine Works
- Innovative Pairing of Beta-Lactamase Inhibitors to Combat Multidrug-Resistant Gram-Negative Pathogens
- Ceftobiprole Joins the Beta-Lactam Squad Against MRSA Infections
PrEP allows for people to simply continue their high-risk behaviors with zero consequences. When they decide to stop PrEP, or become non-compliant, which the majority do eventually, their risk is right back to where it was. The idea that the majority of people without the willpower or concern to ever use a condom will follow all of the screening, monitoring, and consistent usage necessary for PrEP to work is laughable. Sure there are times it’s appropriate (HIV positive partner trying to achieve pregnancy, etc.), and we will see some success in small numbers in certain populations (likely middle/upper income white people.) Maybe we should stop the babying and codify (and enforce) the control measures into law, like in North Carolina (http://reports.oah.state.nc.us/ncac/title%2010a%20-%20health%20and%20human%20services/chapter%2041%20-%20epidemiology%20health/subchapter%20a/10a%20ncac%2041a%20.0202.html).
Wow, overt racism and homophobia. I hope you’re not a health care professional!
Overt racism and prejudice? Right. All I hear about is data on how Blacks and Latinos get HIV/STDs at much higher rates than whites, especially at lower income levels. That’s because they care so much more about taking care of their sexual health? Those same people aren’t going to follow PrEP in an effective way. You can’t have it both ways and cry about racial disparities, but then get angry when they are pointed out. My notion is based on the reverse of the data that already exists…..
And how is my comment in any way, shape, or form homophobic? You know, this is why our country is breaking down politically. Everything people say that you don’t agree with is homophobic and racist. It’s much easier than arguing the facts.
What would you say to an obese hypertensive smoker with an LDL of 220? “I’m not going to give you a statin/ CCB because your high-risk lifestyle should have consequences?”
You would likely face legal liability the moment your patient had a CVA/MI. Like it or not, the day is going to come when a patient under someone’s primary care– perhaps yours– with a litany of risk factors for HIV is going to be infected and then sue his provider.
Your judgement is not a suitable substitute for evidence-based standards of care, which PrEP, approved by the FDA, adopted by the CDC/WHO, and covered by medicaid/care and nearly all private insurance, clearly is.
Second, your statements carry an anger and cynicism that have no place in scientific or evidence-based medical discourse– the literature suggests the opposite of what you say (iPrEX, Kaiser, PRIDE, IPERGAY, etc.). Nearly all of these studies, incidentally, we done in areas of low SES. In fact, iPrEx demonstrated that not only is adherence possible, but that regular interaction and intervention in a poorly educated/ low SES population works alone, regardless of Truvada/adherence.
In our clinics, we have plenty of Black and Latino MSM (and WSM) who are adherent to PrEP; while long term adherence is an issue, from a public health perspective, even a year’s worth of lower HIV risk is worth the effort from a community, if not a clinical, standpoint.
Moreover, the ongoing trials with cabotegravir, an injectable/depot formulation of ARV/PrEP, may ultimately improve adherence problems regardless, should it be successful.
Finally ,it is important to note that many MSM and women of color do not discuss their sexual health beyond acute symptoms because they believe their provider feels exactly how you clearly do. Clinicians, such as yourselves, project a believe that MSM/WSM are incapable or unwilling to mitigate their risk, and are thus deserving of nothing more than a stern lecture, despite the available resources you might bring to bare on a patient you deem more deserving, such as a serodiscordant couple.
The idea that other patients (e.g., Black MSM with low SES) are somehow deserving of the “consequences” of their “high risk behavior” (e.g., HIV/AIDS) is a judgement that is nether true nor one that is the job of a physician to pronounce.
Dr S.
This is the most feisty I’ve seen this forum in a long time. Can we talk about chronic Lyme Disease next week?
Also, based on his notions regarding PrEP, I would love to get David’s thoughts on Viagra. Or not.
David, do you have any data to support the idea that middle/upper income white people are more likely to be compliant with any particular regimen than middle/upper income black people? Latinos? Asians. If you do, please post. If not, you are spreading prejudice, and shame on you.
It is more a socioeconomic factor that does incorporate race to a certain extent, but certainly if you look at white people of lower socioeconomic status you see parallels with blacks latino etc. Having said that the majority of David’s comments are purely hearsay, laymen commentary and most unhelpful. Best to leave interpretation and advice to real doctors, David. Keep your irresponsible non-professional opinion to yourself, please.
I think you’ll find the homophobia in that our society screens and engages in prevention for all types of high risk behaviors (smoking, eating, drinking) but you find a disease that predominantly affects gay males as less worthy of this public health application. You just don’t understand how you are being homophobic, but that doesn’t make it any less the case.
David, you’re the personification on what is wrong with medical professionals and scientists working today. You lack any basic understanding of sociology and modern socio-culture. People of colour are a lot more likely to be suffering through poverty in a western country due to racial discrimination – they are not given a fair opportunity, especially black people.
“A white man with a criminal record is more likely to be hired than a black man without [a criminal record]” – Michelle Alexander, statement from 2016, highly acclaimed civil rights lawyer, advocate, legal scholar. An associate professor of law at Stanford Law School, director of the Civil Rights Clinics.
Being forced into poverty because you’re continuously denied employment, you’re left completely without a support network and the opportunity to receive healthcare, especially if you’re an American. Underfunding in schools, especially in poverty-struck areas, lead to lacking sexual education, and education what HIV is to begin with. This in combination with the inaccessible healthcare (incl. availability of contraception) that is very much available to white wealthy Americans, HIV and teenage pregnancies are a much more common phenomena in poor areas. Your vague statement that “Black people and Latinos catch HIV much more often” is incorrect, unscientific, and pure racism. A persons melanin levels has absolutely nothing to do with their risk of catching HIV. Their levels of melanin does NOT affect a persons disposition which would somehow make them “seek out HIV”, or any other ludicrous similar type of idea. You’re insensitive, delusional, backwards, and very unprofessional.
I second what Adam said – I hope you’re not a health care professional! Come in to the 21st century! Or are you staying in the 19th with Trump?
Additionally, to respond to your statement referring to people of colour becoming “non-compliant” or simply not adhering to treatment schedules, you are once again thinking backwards and ‘black and white’. There are numerous studies that show poverty may lead to PTSD in children and adults. Anxiety and depression to begin with is obvious and practically given part of the life of a child PoC living in a poor area. I’ll assume you’re too unwilling to educate yourself by simply googling “poverty and PTSD”, so here is a publication to start with, fed to you with a silver spoon:
Collins, K., Connors, K., Donohue, A., Gardner, S., Goldblatt, E., Hayward, A., Kiser, L.,Strieder, F. Thompson, E. (2010). Understanding the impact of trauma and urban poverty on family systems: Risks, resilience, and interventions. Baltimore, MD: Family Informed Trauma Treatment Center.
It is common knowledge for any bioscientist or medical professional that depression and many other mental health conditions leads to lack of energy, and of course the inability to adhere to plans, schedules and otherwise general promises – because your health will not allow it. Now I’m assuming it’ll be easy for you to puzzle together 1 and 1 from this, but just to make sure: people of colour in poor areas are at a high risk of suffering from PTSD and other debilitating mental health conditions, which will make it very difficult to find will and energy to adhere to a life saving treatment, especially if the individual is suffering from suicidal tendencies.
I don’t expect you to empathize, David, but you can at least do your (assumed) job and stick to facts and normal reasoning.
As both a physician and a gay man I am very interested in this case report.
David your comment is rife with flat out ignorance and faulty assumptions as to how gay men have sex, use condoms or typically use prep. I myself have an HIV positive boyfriend, we are monogamous and this allows us to have a normal sex life. But before that I was using prep when I was having casual partners and it certainly protected me from one person in particular who was in denial about his HIV status, was high VL and lied to everyone he slept with.
There have only been 3 case reports of transmission despite use of prep in the world despite tens, perhaps even hundreds of thousands of gay men using it. That’s pretty damn good. And I have encountered dozens of gay men in Canada the US and Australia who are using it properly. Your assertions regarding demographics and compliance are also based on bias rather than fact. It behooves ID, sexual health and family doctors like myself to properly educate patients and insist on regular testing (i go every 3 months) while on prep.
My question to those involved in formulation of prep – is the new form of tenofovir (tenofovir alafenamide as opposed to tenofovir disoproxil fumerate) being studied at all or looked at being implanted for Prep therapy? Any reason to think it wouldn’t be as effective? Data published from phase III RCTs shows TAF is concentrated much more in immune cells and lower in the bloodstream, indicating it could be much easier on the kidneys
Steve,
Studies of TAF for PrEP are ongoing. Right now I wouldn’t suggest it, since despite the data you cite which are reassuring, some think the tissue concentrations will be too low for prevention.
Paul
I was married to a ( caucasian ) cardiac surgeon. Unbeknown to me, he was having unprotected sex with a large number of men met on internet. Yes, I got STD’s. Yes, am divorced now. Here you go for your stats:educated white male with high risk behavior, unwilling to change…
Mr. David, I could not disagree more with you. (PS I am an HIV doctor — cis-gender MSM — on PrEP .. so I might know a thing or two about both the medical and the “social” aspects of PrEP)
1- Your point: Blacks and Latinos do not take care of their sexual health — hence have higher HIV prevalence.
** You are perfectly right that there is a significantly higher HIV prevalence in this population — though referring to a recent CID paper ( doi: 10.1093/cid/ciw367) evaluating PrEP uptake: blacks actually have a significantly lower # of sexual partners — reasons of higher HIV prevalence is NOT that they don’t take care of themselves or have MUCH MORE sex; but rather it is * economic reasons * Low access to care * Social Stigma * Lack of insurance coverage.
2- Your point: If they don’t use condoms, then they won’t adhere to PrEP
** Sex shaming the LGBT population does not work. This makes as much sense as saying that women who do not use condoms are not likely to use contraceptives
** condom use is a personal choice and as doctors we are in no place to force people to act a certain way or otherwise they would be banned from using effective and safe prevention methods
** Condoms break
** MSMs who seek PrEP are a very different demographic than those with new infections: have healthcare; urban living; more health engaged and thus are likely to be more adherent
3- Your point: Truvada is a PARTY drug for MSM
** Again it makes as much sense as saying insulin is just a way to allow diabetics to eat things they are not supposed to eat. — so we often tell patients with DM that they are encouraged to decrease their carb intake however if they don’t, we ask them to do carb counting and adjust insulin accordingly (i.e. if you eat cheesecake then increase your short acting insulin dose — does that make insulin a “PARTY” drug? )
4- Your point: middle / upper class white people
** it reflects a lot of prejudice
** You have 0 evidence to back your claim
** Most studies showed that while truvada use (for reasons mentioned above) is lower in people of color than Caucasians, adherence and effectiveness are AS GOOD.
Dr. Sax,
I so enjoy your ID Observations, thank you for this article which is relevant to the work we are doing at my health jurisdiction in supporting people at highest risk for HIV in getting on PrEP. Most people don’t need a lot of support other than finding a doc who is up on PrEP and ready to prescribe (we are not a large city). People are adherent just like my friends and I were with the bcp–meaning some people are just better at taking meds. The motivation is there, and people are so very glad that PrEP is here—HIV+ and HIV- people alike. I am aghast at your unhelpful comments, “David” and hope you are nowhere near anyone who needs medical advice or data interpretation. The draconian attachment you have supplied from the mid 80s is a nice touch,
Thanks Dr. Sax!
I can’t respond to all of your responses as we’re all busy professionals. (Many of you don’t want me to be a physician, so I’ll say I’m a UPS driver to make you feel better.) HIV is a communicable disease. It isn’t cardiovascular disease, it isn’t diabetes, or other diseases that, while sometimes partially “self-induced”, have no transmissibility to others. We don’t have to track down partners of diabetics, or find people who are now diabetic because their friend lied to them about their diabetic status. It’s different. Yes, yes, I’m aware of our ability to often lower the VL to zero, and yes, I’m aware that PrEP can work if followed correctly. I used the example of middle/upper class white people because that’s whose health is always better, and who usually end up making out better. Those of you in the “health care disparities” field are always pointing that out ad nauseum. (You know, the ones who are upset about white privilege.) In the last 10-15 years, white cases have dropped, and black and latino cases have gone up. Anyhow, the way I feel about this personally doesn’t mean I yell this at patients. I am having a discussion in this forum. As per the usual Berkeley-flavored responses, some of them (not all) have been ad hominem attacks. I’m not attacking any one, just expressing my opinions. I thought that was what forums were for. But if it makes Nick Gilpin feel any better for next week’s discussion, I think chronic Lyme is a BS diagnosis the majority of the time, and that Viagra shouldn’t be covered by insurance. 🙂
@David, sorry you are too busy to defend yourself against the impression that you are spreading prejudice. Still waiting for “data to support the idea that middle/upper income white people are more likely to be compliant with any particular regimen than middle/upper income” folks of other races. I do not believe that my question was in any way an ad hominem attack, just asking you to support your contentions empirically rather than by repetition.
@Really Question Mark, the data is very clear: blacks are way over-represented for HIV and STDs. If wealthy blacks aren’t also over-represented, please show me that data. I haven’t see any. (Now STDs are a whole other issue. PrEP doesn’t do anything for STDs but promote more of them. Where is that discussion??) I’m not spreading prejudice.
@David, I am not speaking of HIV prevalence, I am referring to your guess that PrEP would “likely” be successful with “middle/upper income white people.” Lower SES is correlated with poor compliance through a number of obvious factors. If you have no data to support your suggestion that PrEP is more likely to be successful with middle/upper income white people than middle/upper income people of other racial groups, then you are, in fact, spreading prejudice IMO.
And I really would love to hear a PrEP supporter’s take on its lack of STD protection.
@David, I am not taking any position either for or against PrEP, and it is very possible that responsible arguments can be made on either side. I am not an ID specialist, I am just a physician concerned about the possibility of our profession doing harm, in violation of our hippocratic oath. When you say, “I used the example of middle/upper class white people because that’s whose health is always better, and who usually end up making out better,” you are making the precise point that better outcome in that group may be due both to (a) higher SES and (b) the prejudice of doctors who are more likely to offer health-promoting interventions. We have a duty as a profession at the very least to do something about (b), IMO. This is why I am asking you to provide data in support of your statement. If you are not able to provide it (which seems to be the case), I would really like to encourage you to stop making statements of that sort. If you believe that something in what I am saying is ad hominem, please help me understand exactly what you are taking that way.
Why are we discussing if doctors are “for” or “against” PrEP when it has been endorsed strongly by CDC, WHO and CMS ?! This is like saying I am against treatment of Latent TB … You might have reservations about the treatment itself, have situations were you think it’s not the right thing to do.. but IMO no doctor can be “PRO” or “AGAINST” any treatment as a general principle.
I agree with @Scott above — I think every young MSM with new HIV infection, who had not been counseled about PrEP by his doctor, can make a very strong legal argument that his Doctor actually caused harm… As doctors, we should be held accountable not only for the things we do, but also for “what we don’t do” …