
An ongoing dialogue on HIV/AIDS, infectious diseases,
August 28th, 2013
Poll: At $14,105/year, Is Dolutegravir Fairly Priced?
 The recently approved once-daily integrase inhibitor dolutegravir is now in pharmacies and, like every new HIV drug, the price — around $14k/year — has generated some controversy.
The recently approved once-daily integrase inhibitor dolutegravir is now in pharmacies and, like every new HIV drug, the price — around $14k/year — has generated some controversy.
For the record, here are the per-year wholesale acquisition costs of the three FDA-approved integrase inhibitors.
- Raltegravir: $12,976
- Elvitegravir: $13,428 (once disentangled from the price of TDF/FTC)
- Dolutegravir: $14,105
If you add the $12 or 15K for the ABC/3TC or TDF/FTC respectively, you get the total cost of initial therapy. So these integrase-based regimens cost more than TDF/FTC/EFV (22.5K) or TDF/FTC/RPV (23.2K), and less than boosted atazanavir- or darunavir-based regimens, which are around 30k.
Now obviously these are all big numbers — HIV treatment is expensive — but the flip side is that it’s so staggeringly effective that it generally meets acceptable criteria for cost-effectiveness given the huge added years of life.
But incremental cost-effectiveness is another matter — meaning, is the additional cost of one drug over another justified, and/or good value?
Here, then, are two opposite perspectives on the dolutegravir pricing:
- The price is fair, according to the U.S.-based Fair Price Coalition. Dolutegravir is an improvement over currently available options, and the slight premium pricing over raltegravir and elvitegravir/cobicistat is justified. Furthermore, the company met with and heeded community advice on price before the release of the drug — a laudable practice.
- The price is unfair, according to the advocacy group HIV i-Base, which is based in London. The makers of dolutegravir went “for gold” in pricing the drug in the United States, and will therefore severely limit the use of dolutegravir in Europe and likely also in resource-limited settings (though prices in these locations are not yet set).
Your thoughts?
August 26th, 2013
When Eating Guinea Pig, Make Sure to Ask for it Well Done
 I’ve written before about how ID doctors are no fun to have at cook outs, what with our obsession with well-done hamburgers.
I’ve written before about how ID doctors are no fun to have at cook outs, what with our obsession with well-done hamburgers.
Now, there’s another menu item we can berate grill-meisters on, and that’s guinea pig meat:
At least 81 people fell ill from suspected salmonella poisoning after eating guinea pig meat and other foods from a vendor at a Minneapolis street festival earlier this month, health officials said… Scores of people went to Hennepin County Medical Center and Children’s Hospital of Minneapolis with severe gastrointestinal symptoms after eating the tainted food.
So if you decide to order your guinea pig on the rare side, and then get sick, you have no one to blame but yourself.
Because now you’ve been warned.
August 25th, 2013
Death from “Brain-Eating Parasite”: A Reminder of How Little We Really Know
Sometimes it takes a lot to surprise an ID doctor — we who try to make it seem like we’ve seen it all — but certain infections are either so severe (e.g., necrotizing fasciitis from group A strep) or so rare (e.g., endocarditis from Erysipelothrix rhusiopathiae) that even we are startled.
Doubly startling are those infections that score 10 out of 10 on both the severity and the rarity scale.
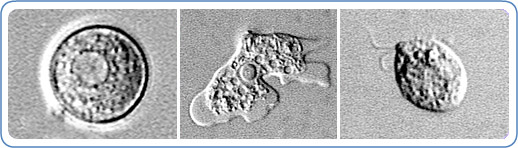
No doubt one such condition is primary amebic meningoencephalitis (PAM), the brain infection that tragically just led to the death of a 12-year-old boy in Florida.
The pathogenesis of PAM is straightforward:
- Naegleria fowleri live in warm freshwater lakes and ponds.
- The parasite enters the body through the nose, usually when someone swims or dives in these waters. (Some cases occur when contaminated water is used for nasal irrigation).
- From the nose, the Naegleria travel back into the brain, causing a severe necrotizing infection that is almost invariably fatal.
However, just because we know how it happens, by no means we know why on an individual level.
Said another way, given the millions of people who swim in warm lakes and ponds each year, why have there been only 31 cases from 2003-2012? Why did this poor boy get sick, but his friends did not?
A case like this is a reminder that, no matter how experienced the clinician, the world of infections and how they cause human disease remains a humbling life’s work.
August 20th, 2013
Underreporting of Lyme Disease No Surprise, but a Big Problem
 In a welcome update, CDC just presented revised data on the number of Lyme Disease cases annually in the United States. Here are the key facts:
In a welcome update, CDC just presented revised data on the number of Lyme Disease cases annually in the United States. Here are the key facts:
Cases reported by clinicians: 30,000
Estimated number of cases using additional information from insurance claims, laboratories, and patient reports: 300,000
Go ahead, check my math — that’s a whopping 10:1 ratio of actual to reported patients with Lyme, highlighting that this reporting is something we clinicians just don’t do very well.
And it’s no surprise to me at all.
Here’s why:
- Clinicians are busy doing other stuff, most importantly taking care of their patients.
- Lyme is one of many reportable diseases — take a look at this list!
- It’s annoying. If you asked 100 doctors and nurses what they like least about practicing medicine, 74.39% would say “the paperwork.”
- The forms can’t be completed quickly, as they request detailed information about dates of exposure and onset of illness, presence of diverse associated symptoms, and evaluations for ancillary diseases. Plus, they’re paper forms — a particular problem in an increasingly web-based and electronic medical record world. As for the specific dates of possible exposure and onset of symptoms? “I just lie,” one PCP told me.
- “Soft calls” won’t get reported at all. Think about the febrile, achy patient in the summer who’s just spent a weekend hiking in the woods, saying ticks were everywhere, then gets treated (appropriately) for suspected Lyme. That may be the billing code the clinician uses, but often as not, no Lyme test is sent.
- No one’s paying for these reports. Forgive the mercenary tone to the comment, but as these folks will tell you, humans are very predictable creatures — give them some incentive to do something, and they’ll often do it, even if the task is unpleasant.
I don’t have an immediate solution to this problem of Lyme underreporting, but it’s important we try to solve it — to quote Paul Mead from CDC, “Lyme disease is a tremendous public health problem in the United States,” and I completely agree.
So let’s look at a disease with extremely accurate surveillance, and that’s HIV.
HIV reporting is tied to receipt of government funds for HIV treatment and prevention. That’s a huge incentive to get the numbers right. If anything, some sites are known to overreport their cases, which is why name-based reporting is such an important accuracy check on the data.
Lest you think that HIV is different because, well, it’s HIV, believe me there are plenty of places where HIV reporting is woefully inaccurate. Back in the mid-1990s, I joined a group from the Harvard School of Public Health to participate in a scientific symposium on HIV in India. There was a reported explosion of HIV cases in certain regions of the country, and their doctors and researchers set up the conference to address this growing problem.
The first presentation was from a public health official representing the government. He showed data demonstrating that the number of cases in India was still relatively small and confined to isolated regions and “risk groups” — mostly commercial sex workers and injection drug users.
The next presentation was from an active ID clinician at one of the largest hospitals in Mumbai. He showed slide after slide demonstrating the ravages of advanced AIDS in diverse populations (emphatically not all commercial sex workers and IDUs) and then finished with a few data slides on cases at his hospital. Turns out that he had seen as many cases at his one site as had been officially reported to the government from the entire country.
When asked how to reconcile his volume of experience with the previous lecture on the national epidemiology, he responded with two other questions.
So why should we report our cases? What good does it do us or our patients?
Once we can answer those questions for Lyme — as we most certainly can with HIV — then the underreporting problem will be solved.
August 12th, 2013
Dolutegravir Approval Signals a Beginning and the End of Something Very Special
As anticipated, the FDA approved dolutegravir today for HIV treatment, the third integrase inhibitor now available.
This was about as surprising as the arrival of Royal Baby Prince George. We knew dolutegravir was coming soon, just not exactly when or what it would be named.
Here’s a short list of the data we have thus far on this drug from various comparative clinical trials:
- Non-inferior to raltegravir in treatment-naive patients.
- Superior (with ABC/3TC) to TDF/FTC/EFV.
- Superior to raltegravir in integrase-naive, treatment-experienced patients.
- The only integrase inhibitor with activity vs virus with raltegravir and elvitegravir resistance.
- Once-daily, no boosting required.
- No food effect.
- Favorable side effect and drug-drug interaction profile.
- Very low risk of resistance with virologic failure.
- Shines your shoes, folds your laundry, and puts out your trash.
Plus, results from another phase III study — vs boosted darunavir — should be available soon.
About the only downsides of this drug are first, that there is currently no single-pill initial treatment (said to be in the works), and second, that the brand name is still another mysteriously unpronounceable choice selected by marketing gurus undoubtedly paid much more than we are.
(“Tivicay.” Let’s see, is it Tivi-SAY, or Tivi-KAY? Or TI-visay or TI-vikay? Or maybe it’s a long I on the first syllable, as in “tie …” Gosh, who knows. Better call the people who know how to say Intelence and Stribild and Fulyzaq.)
Pronunciation aside, this is the beginning of this extraordinarily promising antiviral agent.
But it’s the end of a remarkable stretch of HIV drug development, one that started in 2006 with darunavir, then marched through with maraviroc, raltegravir, etravirine, rilpivirine, and elvitegravir. The availability of these drugs, now with dolutegravir, means that pretty much anyone who takes their medications will achieve virologic suppression.
Because after the tweak of tenofovir — TAF — what’s next?
August 7th, 2013
Occupational Post-Exposure Prophylaxis (PEP) Guidelines Updated — And They Are Clear and Sensible
 Good news here — the United States Public Health Service has issued new national guidelines for management of occupational exposure to HIV.
Good news here — the United States Public Health Service has issued new national guidelines for management of occupational exposure to HIV.
Authored by an expert panel, these updated occupational PEP guidelines replace the (woefully outdated, sorry, had to write that) previous version, which dates back to 2005.
On a quick read-through, despite the density of print, the new guidelines are excellent and sensible, providing much needed clarity to an often confusing and anxiety-provoking clinical situation. They are quite similar to the NY State Guidelines, which have acted as a nice guidance as we awaited these national recommendations.
Here are some of the key recommendations.
- Clinicians may use any validated testing options for evaluating the HIV status of the source patient. This includes point-of-care rapid tests.
- No need to rule out “window period” in the source patient unless acute HIV is suspected clinically. Good to see this explicitly stated.
- PEP regimen of choice: TDF/FTC plus raltegravir for 4 weeks. Many alternative regimens are listed, including the single-pill TDF/FTC/EVG/c combination, which may be useful for non-compliant patients provided there are no significant drug-drug interactions. Full details here.
- No recommendation to use two drugs for lower-risk exposures — it’s all or nothing.
- Expert consultation recommended in several scenarios — for example, delayed (>72 hours) report of exposure, needle stick of unknown source, possible HIV resistance in source patient, pregnancy or severe illness in exposed patient. However, seeking expert consultation should not delay starting PEP.
- The follow-up period for exposed individual can be shortened to 4 months (from 6) if a 4th generation combination HIV p24 antigen/antibody test is used. There isn’t a single exposed health care provider who wouldn’t want this shorter follow-up option.
I especially like this last point — this will greatly decrease the period of anxiety in those exposed! Hope these guidelines provide motivation for hospital labs to update to their HIV screening assays to the 4th generation tests, if they have not done so already.
Now about that gestation period of these guidelines …
August 6th, 2013
Nelson Cruz and Yet Another ID-Baseball Link
Texas slugger Nelson Cruz is one of the Biogenesis gang just suspended from baseball for use of performance-enhancing drugs (PEDs).
For those who care about these things, he’s also probably the most important player from the banned list, since he’s 1) very good and 2) on a team in contention for a playoff spot.
For those who don’t care about baseball, we have this from Cruz himself:
From November 2011 to January 2012, I was seriously ill with a gastrointestinal infection, helicobacter pylori, which went undiagnosed for over a month. By the time I was properly diagnosed and treated, I had lost 40 pounds. Just weeks before I was to report to Spring Training in 2012, I was unsure whether I would be physically able to play.
Now with the caveat that we ID doctors are woefully uneducated about all things helicobacter, it’s pretty clear that guidelines for treatment of H pylori don’t include testosterone, growth hormone, and whatever other garbage Biogenesis was peddling.
But could they make you a better right fielder?
August 1st, 2013
Poll: Will There Be A Shortage of HIV Providers?
 Over on NEJM Journal Watch — love that new name — I reviewed a paper on the demographics of people living with AIDS in San Francisco.
Over on NEJM Journal Watch — love that new name — I reviewed a paper on the demographics of people living with AIDS in San Francisco.
Bottom line — more than half are now older than 50.
Implication — that’s so old!
First, it really isn’t, unless you compare it to the dismal era 20+ years ago, when so many of the sick and dying with AIDS were young men and women. Let’s face it, that was one of the true horrors — maybe the horror — of this new disease.
Second, this aging of the HIV population is of course really a good thing, since it means fewer people are dying of AIDS.
Third, what does it say about us, the HIV providers? The doctors, nurses, PAs, PharmDs, social workers, case managers, etc. who have been at this for quite some time now.
Obvious answer: We’re getting older too. Even older than 50.
(Yes, for the record, you could say that I’m speaking from personal experience here.)
In fact, this paper prompted one of my colleagues to ask me about our successors. What happens when we oldsters decide to do something else? Who’s going to take our place?
I’ve heard anecdotally that in some parts of the country it’s been difficult to attract young clinicians to HIV/ID, with multiple reasons cited — not enough revenue, HIV/AIDS lacks the drama it used to have, the patient population has changed, all the young people are now interested in only international work, there are no good jobs available.
Let’s take these one at a time:
- Not enough revenue: I guess there is some truth to this, especially in a health care system that values volume and procedures over complexity. But this has hardly changed, so it’s not as if anyone went into HIV/ID primarily for cash to begin with. Hey, this is not orthodonture, folks!
- HIV/AIDS lacks the drama it used to have: Certainly fewer premature deaths means less drama — but is this is the kind of drama anyone really wants? I wouldn’t trade the current HIV treatment era for the early 1990s in a million years.
- The patient population has changed: In fact, it really hasn’t — HIV/AIDS has disproportionately struck gay men (all races/ethnic groups) and heterosexual racial/ethnic minorities for decades now. There are fewer new infections from injection drug use and hemophilia, but that’s about it.
- All young people are now interested in only international work: Yes, some of the trainees are truly committed to establishing a research and/or clinical base in regions that have a far worse HIV/AIDS problem than we do. But for many this initial enthusiasm fades once they realize how difficult it is to do this successfully — especially while simultaneously trying to start a family. Which means they also want to work here, or even predominantly want to work here.
- There are no jobs. Well, there will be when we retire — that’s the point of this discussion!
So is it true that we won’t be able to find new HIV/ID providers to care for HIV patients when we stop doing it?
July 29th, 2013
CROI 2014: March 3-6, Boston, Massachusetts, USA, North America, Earth
Ok, that’s one mystery solved.
(We’ll do our best to have the ice and snow cleared away by then, but no promises — New England weather is the very definition of unpredictable.)
And now that we know the CROI 2014 dates, here’s some good news: I hear they’re working on getting the 2015 dates squared away as well.
If so, good work, new CROI organizers!
Keep an eye out for further details (deadlines, etc) here.
(Thanks to an un-named but very reliable source for this, who gave permission to share the info.)
July 23rd, 2013
Guess it Wasn’t the Acyclovir After All
Big news in baseball land is that superstar Ryan Braun has been suspended for the rest of the season for using performance enhancing drugs (PEDs).
And why is this information in an Infectious Diseases blog? Three main reasons:
- When Braun first got nabbed for PEDs in 2011, it was widely rumored it had something to do with treatment for herpes. Not surprisingly, I was confused about this, but reasoned that maybe — just maybe — it was due to an interaction between acyclovir and endogenous testosterone production. Pretty weak, I know.
- Braun then got the suspension dropped because the urine specimen wasn’t handled properly. In hindsight, Braun made some astounding comments after getting off, but no mention whatsoever of acyclovir.
- I will use any excuse imaginable to write about baseball.
Admittedly, the last one is probably the biggest factor here.
Ah, for a simpler, more innocent (!?) era …

Paul E. Sax, MD
Contributing Editor
NEJM Journal Watch
Infectious Diseases
Biography | Disclosures | Summaries
Learn more about HIV and ID Observations.