
An ongoing dialogue on HIV/AIDS, infectious diseases,
May 10th, 2021
Goodbye, Physician’s First Watch — We’re Really Going to Miss You
WPA travel poster (1939) has nothing to do with this post, but I like it since everyone hates mosquitos, especially ID docs.
One of the great joys of life is working with great people, and for me, this includes frequent interactions with several skillful medical editors. They scan these posts for typos and awkward sentences, and warn me when I inadvertently include a copyrighted image or an inappropriate video.
They also worked, until recently, for Physician’s First Watch, which sent out daily emails highlighting the top stories in medicine — published papers, conference highlights, policy changes, new guidelines.
For practicing clinicians too busy to keep up with the voluminous medical literature and breaking news, this service was absolute gold — how else would an Infectious Diseases doctor learn about (yet another) negative vitamin D study? The latest on how to manage back pain in outpatients? Or understand that the USPSTF has come out with (yet another) recommendation against screening for a certain disease?
(Those USPSTF guys sure are tough. Wonder if you have to take a standardized skepticism test before joining this group, with only those scoring in the 99th percentile allowed in.)
That the First Watch newsletter came from a trusted source, with the appropriate references readily linked, only added to the value. You never felt like it was a thinly veiled marketing platform, or clickbait. Here’s What the Grouchy USPSTF Panel Does in Its Free Time — and You’ll Never Believe It.
Physician’s First Watch also kept me updated in my own field, Infectious Diseases — in particular advances outside of my primary areas of focus. Recent examples included a systematic assessment of delayed antibiotic prescribing in the outpatient setting and an observational study comparing amoxicillin-clavulanate and metronidazole plus a fluoroquinolone.
Alas, Physician’s First Watch ceased publication on April 29th — and the medical world mourns. Email from a Dr. Frank Domino, a primary care physician:
Hey Paul —
Why did NEJM stop First Watch? It was awesome! Kept me up to date better than anything, and I used it as a teaching tool with students all of the time.
Frank
We agree, Frank. It was regular breakfast table conversation fodder for both my wife (a practicing pediatrician) and me.
As I understand it, the decision was purely a business one, as the quality was always superb. But publishing in general, and medical publishing in particular, is going through a very unstable time. It’s no secret that many online and other “free” electronic endeavors have not been able to generate revenue from their content, a problem exacerbated during the COVID-19 pandemic. Here is a superb review of why some of these sites have either shifted to a subscription model or shut down entirely.
But one thing is clear, at least for now (looks over his shoulder) — I’m going to continue writing on this site. Am enormously grateful to NEJM Journal Watch for the opportunity to write this blog or column or newsletter, or whatever you want to call it. I also greatly appreciate all the regular readers, and comments, and suggestions, and feel like we’ve built a wonderful ID-oriented community that welcomes anyone interested, ID-trained or not.
For those who relied on Physician’s First Watch for notification about new posts, that’s not going to work anymore. But you can subscribe by entering your name and email address in the Subscribe box at the end of this post or in the column to the right, and confirming that you want a subscription — then shazam, just like magic, you’ll get an email when a new post appears. Don’t worry, we won’t share your name or email with anyone.
I’ll continue to cover the latest on ID, HIV, and while it’s still with us, (deep breath) COVID-19 — along with other general ID and non-ID topics, and the occasional silly digressions. Here’s a summary of the various things covered over the years.
Who knows? One of these days I might come up with a more interesting title — suggestions still welcome!
Subscribe to this blog!
May 3rd, 2021
Some Colleges Require COVID-19 Vaccination — Why Don’t They All?
Horse Feathers, 1932. Paramount Pictures.
Each time a college announces that it requires that students be immunized for COVID-19 to attend in-person classes or to live on campus, I do a little cheer. Sometimes it’s accompanied by a happy dance — especially when it’s right in my neighborhood.
Why?
Because ever since the pandemic started, carefully done epidemiologic studies consistently show that older teens and young adults have the highest incidence of infection.
This fact might be counterintuitive, since older people bear the disproportionate share of severe disease. As a result, the media quite regularly gets it wrong, by reporting each time when cases surge anew that “this time it’s different — it’s young adults.”
Nope. It’s always been younger adults. They just don’t get as sick. And during the first wave in early 2020, with testing severely limited, we could only test the sickest people — sometimes only those who came to the hospital. Infections in younger people went undiagnosed, since most cases were mild or asymptomatic.
But three key points about COVID-19 in young people should strongly favor mandatory college immunization. First, some young adults get quite sick indeed. Some have lengthy post-COVID symptoms that keep them out of school or work for weeks or months. Some get hospitalized. Some even die, with tragically so many years of life lost.
Second, outbreaks on college campuses can be large, disruptive, and enormously resource-intensive to control. The testing and infection control protocols vary from school to school, but all are costly in both time and dollars.
Finally, young adults with COVID-19 play a key role in perpetuating the epidemic. Mild disease is still contagious, of course, and communities with in-person higher education experienced an increase in COVID-19 incidence, suggesting that infections in students lead to transmissions both on campus and off.
Indeed, vaccinating college students may be a critical strategy in bringing the pandemic under control. Health economist Dr. Zoe McLaren summarized this benefit nicely in this thread:
Young people have a lot more power to end the pandemic than they might realize. Some modeling studies actually show that, under certain conditions, high vaccination rates of people 16-24 could end the pandemic more quickly than vaccinating the vulnerable. 5/8
— Zoë McLaren, Ph.D. (@ZoeMcLaren) March 21, 2021
She kindly referred me to this modeling study, which demonstrated the powerful public health benefits of vaccinating younger adults. Note that the effects would be even bigger than in the study, as the vaccines turned out to be more effective at blocking infection than the authors estimated at the time.
Some might wonder why the rate COVID-19 is so high in teens and young adults. But those who are parents of kids this age, or even better have an accurate memory of their 15-25-year-old self, will not be surprised. When you’re this age, socializing with friends isn’t just a leisure activity — it feels like breathing oxygen, necessary for survival. It’s during this socializing that we develop our identity, affiliations, and friendships, test our independence, and explore the broader world as an almost-adult.
Is it any surprise that this age group would have the hardest time with social distancing? While many of us older types, already paired-off or settled or both, haven’t dined out in months, a college student who starts a new semester in a dormitory or off-campus apartment isn’t likely to sit at home alone all semester, ordering groceries online and avoiding all group dining. And this doesn’t even get into classes, study sessions, sports, concerts, Greek life, or romance.
So what’s blocking the universal requirement for vaccination before on-campus classes or living? After all, don’t most universities require documentation of several immunizations already? Yes. COVID-19 is a far greater threat to personal and public health than many of these other vaccine-preventable illnesses.
One frequently cited obstacle is that these vaccines are not yet fully FDA-approved. True — but this is just a technicality:
Harvard Law professor Glenn Cohen, who teaches health law and bioethics, said there’s no legal reason colleges wouldn’t be allowed to require COVID-19 vaccinations. It makes no difference that the shots haven’t been given full approval, he said, noting that many colleges already require students to take coronavirus tests that are approved under the same FDA emergency authorization.
Already nearly 200 universities have issued a ruling requiring that students get a COVID-19 vaccine. Medical exemptions, of course, are permitted, but based on the safety profile of the vaccines, should be infrequent. (Thanks to Benjy Renton and his invaluable site for that link — he’s been providing terrific coverage of COVID-19 and higher education for months.)
So go for it, colleges and universities. Make the COVID-19 vaccine a requirement for on-campus learning and living, even offer it on-site for those who can’t get it at home. You have my 100% support.
Groucho, Harpo, Chico, and Zeppo agree.
April 25th, 2021
The Decision on the Johnson & Johnson COVID-19 Vaccine Surprised Me — Here’s Why
The “pause” on the one-shot Johnson & Johnson (J&J) COVID-19 vaccine is over. Based on a further review of safety data that occurred on April 23, both the CDC and the FDA said the vaccine may resume here in the U.S., provided the label includes a warning about a serious, but rare, side effect — thrombosis with thrombocytopenia syndrome (TTS).
I confess this decision surprised me. My hunch was that they would advise limiting the vaccine in the U.S. to women older than 50, with no age criterion for men. Instead, it’s now available for all.
This was no doubt a tricky decision, one reflected in the 10-4 vote of the Advisory Committee on Immunization Practices (ACIP). When experts disagree, I find it useful to list those things we all can agree on:
- These are not your typical blood clots. TTS bears a strong resemblance to heparin-induced thrombocytopenia (HIT), with low platelets and development of antibodies to platelet factor 4. This “consumptive coagulopathy” has distinctive clinical features, is challenging to manage, and should not be treated with heparin — which can worsen the disease.
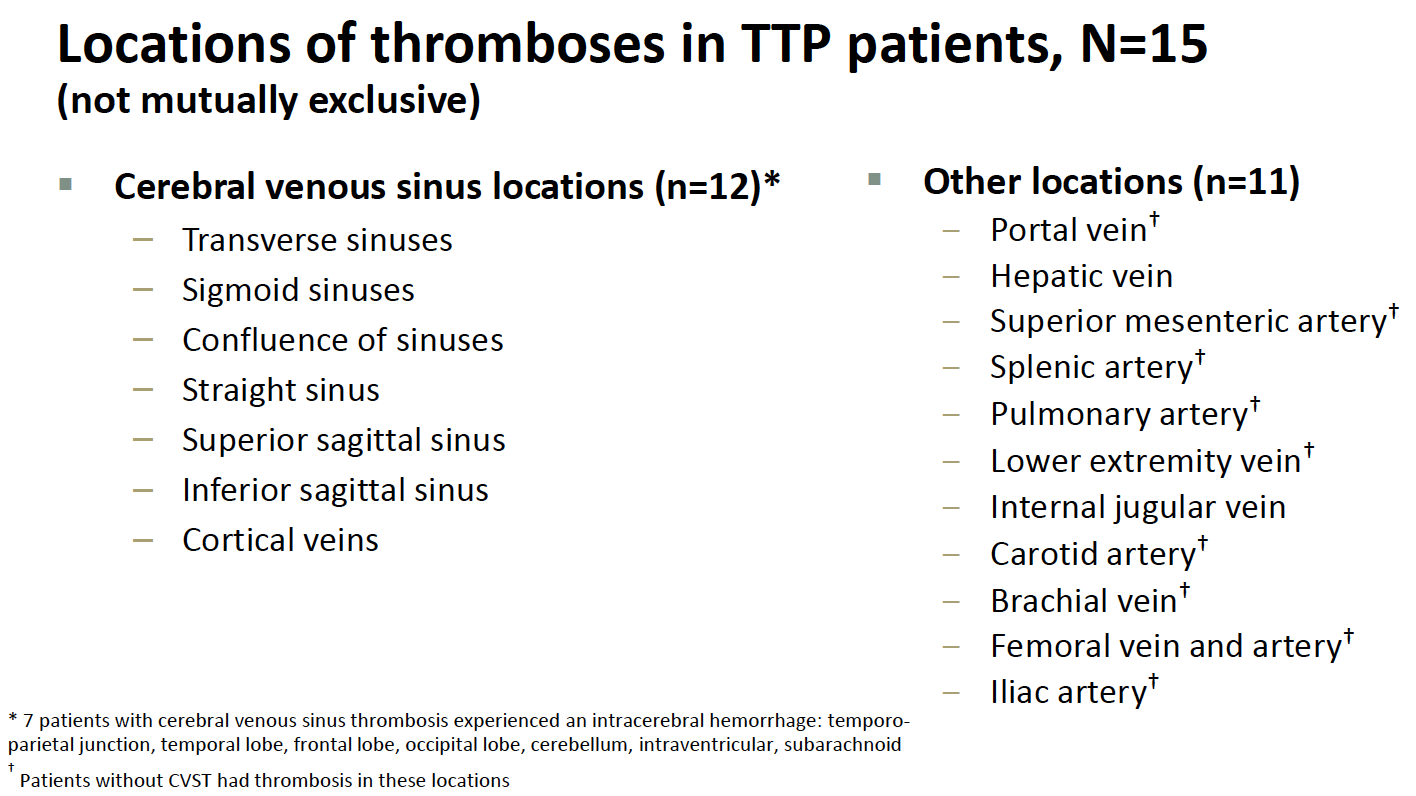
- The cases are very serious. Venous thrombotic events vary widely in severity; the clots in these TTS cases occurred in particularly bad anatomic locations, most commonly in the cerebral venous sinuses. Cerebral venous sinus thrombosis (CVST) can lead to permanent neurologic disability, require intensive care, or even be fatal. In the TTS cases, clots also occurred in other sites, and in the arterial system. From Friday’s ACIP meeting:
- They are rare. Nearly 8 million people have received the vaccine, and 15 of these distinctive clotting events occurred, for a rate of around 1 case per 500,000 people vaccinated. Additional cases may come to light, and apparently, around 10 are under investigation.
- The risk is higher in younger women. Thus far, all the cases occurring since the emergency use authorization (EUA) have been in women. The median age was 37 years (range 18–59). For women aged 18 to 49 years, the estimated TTS rate is approximately 1 per 140,000 doses — and potentially higher if more cases occur in this age group among the 10 or so being investigated. Plus, in hindsight, a 25-year-old man likely had a similar syndrome during the clinical trial.
- They occurred shortly after the vaccine. Median time to symptom onset was 8 days (range 6–15 days).
- Similar thrombotic events occurred with the AstraZeneca COVID-19 vaccine. This adverse effect is the primary reason some countries slowed the rollout of this vaccine globally or limited who should receive it. (The vaccine is not used in the U.S.) With the AstraZeneca vaccine, a broader demographic appears to be at risk. Both vaccines use an adenovirus vector strategy to deliver the SARS-CoV-2 spike antigen.
- No cases of TTS have yet occurred with the mRNA vaccines. While thrombotic events have been reported after the Pfizer or Moderna vaccines, none of the cases had low platelets or the other distinctive characteristics of TTS. Given the nearly 200 million doses of these vaccines already administered in the U.S. — with millions more globally — these are highly reassuring safety data.
- The J&J vaccine has several favorable characteristics. As a one-shot vaccine with less stringent storage requirements than the mRNA vaccines, it theoretically would be easier to give to a broader — and sometimes disproportionately at-risk — population. Specifically cited in the ACIP meeting included the homeless, rural residents, people in prison, disabled, homebound, or those with limited access to healthcare.
- We have a sufficient supply of mRNA vaccines to vaccinate all eligible adults in the United States. Given what India is going through right now, just writing this breaks my heart — but it’s true and must be considered in the risk calculation of using the J&J vaccine. Hence while the favorable characteristics of the J&J vaccine would make vaccinating the U.S. population easier, it may not be required.
- COVID-19 case numbers are falling in most of the United States. Even Michigan, the state with the recent marked surge, is fortunately now showing a sharp decline in case numbers. Again, this is critical when thinking about the risk calculation for someone choosing whether to be vaccinated and when.
The process by which safety issues come to light with these vaccines is truly impressive. These rare events triggered a thorough investigation, one in full public view with all the data shared. That’s a real win.
But let’s now consider an otherwise healthy young woman who wants a COVID-19 vaccine.
Give the availability of the mRNA vaccines, the falling case numbers nationally (and hence her reduced risk of disease), and the rare — but extremely serious — side effect of TTS that might occur with the J&J vaccine, under what possible circumstances should the J&J vaccine be the recommended approach?
If it’s a matter of convenience, I’d say it’s worth spending the time educating about how to get the two shots and avoiding the small risk.
If it’s a matter of lack of mRNA vaccine availability, I’d say fix the supply issue or outline where an mRNA vaccine is available.
But now? It’s possible that this young healthy woman might end up getting the J&J vaccine. And while the odds are overwhelmingly in her favor that everything will be fine, in practice, this would be giving a vaccine with a recognized safety issue when two highly effective and safe alternatives exists.
And the warning? I worry about women who lack the medical literacy to fully understand it, or the cultural authority to question what is being offered to them, or the forthrightness to request alternatives — or all of the above.
And that can’t be right.
April 19th, 2021
Is It Time to Eliminate Outdoor Mask Mandates?

Louie checks out our local town policies.
I do the morning dog walk in our house. And every day, I put on a mask before going out, just as I have since March of last year.
As the data accumulate on the dynamics of SARS-CoV-2 transmission, it’s definitely time to ask this question — why am I still doing this? After all, it’s just Louie and me — and even he’s wondering.
It’s generated some interesting dialogue between the two of us:
Why are you doing that? he asks me each morning. Who are you protecting?
Good questions, Louie!
It’s true, I’ll briefly pass an occasional person on the street or sidewalk. But they’re not going to get COVID from me, or the reverse. That’s not how this works.
Even if I, as a fully vaccinated person, were asymptomatically carrying SARS-CoV-2 — already exceedingly unlikely on any given day — the virus would be rapidly diluted by the extraordinary ventilation conferred by just being outside.
And while the vaccines aren’t 100% protective of me — nothing is, sports fans — they are amazingly good. Got to love these recent CDC data, interpreted by indefatigable COVID-19 optimist Dr. Monica Gandhi:
When CDC says <1% vaccine breakthroughs, let's be specific & say 0.008%. And in terms of severe disease, 0.0005% and in terms of deaths, 0.0001%. And Dr. Fauci said severe disease in elderly with other health problems to NPR. Reduce hesitancy by optimismhttps://t.co/mYLQ7G8psi https://t.co/MsQJwGPtkT
— Monica Gandhi MD, MPH (@MonicaGandhi9) April 17, 2021
With COVID-19, the most intensely studied viral respiratory tract infection in over a century, it’s worth emphasizing that clear documentation of outdoor transmission has been a challenge — and it’s not for lack of trying. In such rare cases, it’s often impossible to disentangle the indoor activities accompanying the outdoor events as contributing to the risk.
Or the people were crowded together outside, facing each other and interacting. Or exercising together and breathing heavily.
Transmissions do not take place between solitary individuals going for a walk, transiently passing each other on the street, a hiking trail, or a jogging track. That biker who whizzes by without a mask poses no danger to us, at least from a resipiratory virus perspective. Read more about the safety of being outside in this excellent piece by Shannon Palus, which also questions the need for masking outside — generating quite the heated commentary, as I anticipate this post will also.
But what about the community solidarity engendered by wearing a mask outside in public? Isn’t this worth something? A way of showing that I’m 100% part of Team Mask?
Maybe — certainly there’s a strong component of this messaging among the highly adherent mask wearers here in Boston. But this performative aspect of outdoor mask-wearing has a downside, too.
You might think you need to wear a mask while walking me in the morning to set a good example for others, said Louie the other day.
But really you might be misleading people about how the virus is transmitted.
Wise words, dog of mine! (He’s very articulate.)
Here’s a bold proposal — let’s make public policy based on our best understanding of the science of SARS-CoV-2 transmission:
Dangerous — crowded indoor spaces with poor ventilation, in particular with unmasked individuals talking, shouting, singing. Wear a well-fitted mask until case numbers are down and more people are vaccinated.
Safe — outdoors, especially while distanced. Masks only needed for lengthy interactions with others at close distance.
Some might wonder if this is too nuanced a message — the “people will get confused” argument.
Give them more credit than that, says Louie. If I can understand it — and I’m a dog — so can they.
He’s got a point, it’s not that hard. We’ve learned so much since the terrifying days early in the pandemic — why not share what we’ve learned and eliminate mandates that no longer make sense?
To wrap up, Zeynep Tufekci kindly shared her thoughts on this issue. She’s been fighting something she’s called “beach scolding” for over a year now. It’s when public health officials and the media shame people or even worse prohibit outdoor activities — when they should be encouraging them since they’re so much safer. Examples — the dreaded yellow police tape outside the park or on the benches, the swings removed from the playground, the beaches and lakeside trails closed.
In a way, it relates to outdoor mask mandates:
Sometimes people invoke the precautionary principle or what’s the downside argument to argue for universal masking outdoors. However, the precautionary principle is not necessarily appropriate after a whole year of epidemiological data showing little to no transmission outdoors outside of sustained close contact: precaution is what we do when we don’t know the answer, not something we invoke to continue doing things on autopilot.
Plus, there is a very important downside that’s not being considered sufficiently: by mandating or normalizing masks outdoors at all times, we are miscommunicating about the real risk factors—indoors, especially if they are crowded and poorly-ventilated—which means that even a full year after the pandemic, people are not being properly informed about where and how they should increase their vigilance.
It’s fine to tell people to continue wearing masks outside especially if they are unvaccinated and are about to engage in a sustained interaction at close distance, especially if it involves higher aerosol emitting activities like talking, yelling or singing, but it’s time for the excessive masking outdoors, and especially mandates, to go.
Bravo. Looking forward to seeing more outdoor faces soon.
April 11th, 2021
Poll: Will This Video Change Anyone’s Mind About Getting a COVID-19 Vaccine?
Watch this video. It’s a minute long:
I first heard about the video because, as mentioned before, I play in a regular poker game with a group of smart friends. Naturally, the in-person game, which started sometime in the early days of the 21th century, has been on hold since March of last year. One can barely imagine any activity more efficient for respiratory virus transmission than a bunch of people clustered around a small table, playing cards, chatting, eating snacks, and consuming beverages.
But we still play online, which one of our players estimates is approximately 64.7% as fun as the face-to-face game. So it’s quite appropriate that the video was sent around to all of us this past week after one of our online games. It came from Mo, a skillful player whose name sounds like it’s right out of a movie based on a tricky poker hustle.
I don’t think he expected this response from Mark (another poker expert) or me (a relative hack):
Mark: Just a big tech conspiracy.
Me: I can feel the microchip right under my biceps muscle.
Mo: Such cynics! Of course advertising by definition is supposed to manipulate you. But what’s wrong with being made to feel good about something good?
I agree this video is brilliant advertising and did make me feel good. It’s downright wonderful. The stark simplicity (always an enticing strength of a Google search), the music, the sound effects, the use of different languages, and, most importantly, the broad range of activities put on hold now possible again with vaccination — they all work together to convey a powerful and moving message.
No wonder some of the YouTube commenters wrote that they cried while watching it.
But will it convince anyone to get the vaccine who is otherwise not doing so?
Not so sure about that, but suspect not many. Why?
Our vaccine-eligible population, at least here in the United States, falls into various groups:
National Library of Congress
1. Most want the vaccine. They can’t wait. They signed up the very first day they were eligible. Or drove long distances to find a pharmacy that had extra shots. They watched the vaccine criteria in their states closely, hoping they and their loved ones would be candidates. Before then, they dropped in at end of the day at vaccination sites, eager for leftovers. When finally getting the vaccine, they were overwhelmed with emotion, gratitude, and relief. Maybe they took a vaccine selfie. Then they helped others navigate the process.
In short, this group loves this one-minute video. (So did all the poker players, for the record — including Mark.)
2. Some are on the fence because of a medical reason. They worry the vaccines are too new. That they might make their underlying autoimmune disease worse. Or they have a history of terrifying, life-threatening allergies to medications and maybe even vaccines. Or they are pregnant, or planning pregnancy. Or they had a rare, very severe side effect in the past to another vaccine, and worry these will do the same.
(All us ID doctors have been asked about people with Guillain-Barre syndrome after a flu shot and whether they can safely receive a COVID-19 vaccine. We say it’s safe — at least as far as we know.)
These are all legitimate concerns, for which there are no easy answers. People in this group might find the video well done, but it’s unlikely to alter their decision-making.
3. Some won’t get the vaccine since they come from marginalized groups. They might know about how the medical community excluded them from research in the past. Or conducted unethical studies. Or treated them poorly in a clinical context, so they inherently distrust our messages. Or they don’t speak English, and no culturally appropriate vaccine information is available. Or they have limited access to regular medical care.
I suspect this group won’t even see this video — where is it being distributed? — or if they do, they will distrust it.
4. Some await herd immunity, so they believe if they wait long enough, they won’t need to get the vaccine — ever. They are analogous to the parents who seek out “non-medical exemptions” for their children so that their kids won’t have to get the recommended childhood immunizations.
This group — particularly selfish, I should add — will watch this video and hope that it will convince others to get the shots.
5. Some are anti-vaxxers, or conspiracy theorists, or political extremists, or some combination of these factors. They will see in this video various hidden messages proving that the vaccines allow 5G mobile networks to take over their brainwaves.
I look at these five groups, and wonder — is this video going to sway anyone from Groups 2-5?
Will it, as cleverly put by Tom — another poker mate — “move the needle?”
What do you think? And why?
April 4th, 2021
More Excellent News on COVID-19 Vaccines — and Baseball Gets a Policy Right
A Joyful Easter, 1900. New York Public Library.
Big announcement this week from CDC, saying that people who have been fully vaccinated for COVID-19 can safely travel.
Of course many didn’t need this permission, as data increasingly show the vaccines not only powerfully protect you, but protect others. But having official endorsement from our cautious federal health agency surely means the data are especially strong.
For the record, it’s worth highlighting two recent bits of extremely good news on the vaccine front:
- The Pfizer vaccine continued to provide high-level protection at least 6 months after immunization. Over 90% effective in preventing any symptomatic disease, and 100% in preventing severe disease. Why is this important? The clinical trial started during the summer of 2020, which means these data take us through the winter surge in cases that occurred globally. Furthermore, the vaccine was just as effective in South Africa, where the more transmissible B.1.351 variant is highly prevalent.
- Prospectively collected data from the CDC show that people who received the mRNA vaccines were 90% less likely to get infected. The study included nearly 4000 front-line workers who were tested regularly by RT-PCR, even without symptoms, and confirms similar data collected in the United Kingdom and Israel, also with large sample sizes. Here’s why these data are important — fewer people with infection means fewer who can infect somebody else:
Amazing prospective @CDC data reinforcing that these vaccines prevent disease *and* infection — and hence reduce the risk of transmission.
Remember, fewer people with infection means fewer who can infect somebody else.
Let's get vaccinated ASAP! https://t.co/k9wl9Tsrmp
— Paul Sax (@PaulSaxMD) March 29, 2021
Many (including me) have always thought that it would be highly unusual if these powerfully effective vaccines failed to reduce transmission risk — now we have multiple lines of evidence that indeed they do. It may not be 100% — nothing is — but it’s a lot. To quote Dr. Neil Stone, “it takes a special kind of pessimist to believe that Covid vaccines won’t significantly reduce transmission of virus.”
We don’t want to be that kind of pessimist.
Why should we stress the highly favorable nature of the vaccine effectiveness data, both for personal health and the health of others? This will help many of those who are on the fence about whether to get vaccinated make the right decision — which is emphatically to get a COVID-19 vaccine. This will become increasingly important when supply of the vaccines exceeds the demand, and any adult will be eligible for immunization.
But what if this isn’t enough? Should we proceed with vaccine mandates in certain settings? Especially in high-risk transmission jobs, such as healthcare, where vaccination will both protect our patients and make the work environment safer for others working in the same setting?
As noted in this excellent concise review entitled “Should healthcare institutions mandate SARS-CoV-2 vaccination for staff?”, the question raises several challenging ethical questions. The piece covers the pros and cons, ultimately concluding that “mandates may be ethically permissible in select circumstances.” It also notes that from a practical perspective today, the current “emergency use authorization” of the vaccines makes them technically still experimental, hence a mandatory immunization is “legally and ethically problematic.”
I would argue, however, that with the pandemic still very much ongoing — COVID-19 cases are up substantially over the past few weeks — individual company policies can strongly encourage vaccination by making it the ticket to greater on-the-job benefits, flexibility, and freedom.
A carrot, not a stick.
An example? Here’s what Major League Baseball did, in a move this ID doctor and rabid baseball fan 100% supports:
Major League Baseball is getting back to normal. Players can now travel with their families. They can go to restaurants. They can play cards and move around on planes and buses. They can use whirlpools and saunas in the clubhouse. And they no longer are required to wear a mask on the bench or in the bullpen. However, teams are first required to have at least 85% of their players and staff fully vaccinated … Plus, these new protocols only apply to those who have been fully vaccinated.
In other words, if you and enough of your teammates agree to get vaccinated, here’s what you get in return — freedom! It’s analogous to CDC saying that fully vaccinated people can safely travel.
Despite the increase in cases, the pathway out of the pandemic looks brighter all the time. And it’s these amazing vaccines that will lead us there.
Spread the word.
March 21st, 2021
If You Want Thoughtful and Accurate Predictions About COVID-19, Zeynep Tufekci Has the Answers
Pufferfish, from United States Exploring Expedition (1838-1842)
The future ain’t what it used to be, said one very wise man.
He might have also said, It’s difficult to make predictions, especially about the future, but alas we’ll have to credit that profundity to someone else.
Still, both these statements embody the insurmountable difficulty of making accurate predictions — a problem starkly evident during pandemic times. How many times have we watched people give conflicting views of when, or how, this thing is going to play out, even in the short term?
Two recent examples come to mind. Dr. Mike Osterholm, Director of the Center for Infectious Disease Research and Policy at the University of Minnesota, repeatedly warns of an additional surge this spring as more contagious variants take hold. This headline calls him “Dr Doom.”
On the flip side, Dr. Marty Makary from Johns Hopkins wrote in mid-February that we’ll likely be mostly done with COVID-19 in April — which, if I’m doing the math, starts 11 days from now. They can’t both be right.
Our ability to make accurate predictions is highly flawed, dependent on innumerable forces we can only begin to understand.
We base these predictions on our background, our education, our knowledge base, plus an unconscious force that sends them in various directions — optimistic or pessimistic, confident or timid, contrary or mainstream.
The bold ones get the most attention, especially if backed by impressive credentials. If Larry Summers says we’re heading into ruinous economic territory with the stimulus package, who am I to question him? Or Janet Yellen, who predicts the exact opposite?
Enter Zeynep Tufekci — sociologist, computer programmer, and Associate Professor at University of North Carolina. You might expect an epidemiologist, or infectious diseases specialist, or virologist to have the best record in laying out the most likely way forward as COVID-19 continues its march around the globe, now 15 months in. But again and again I have found hers to be among the most logical voices, mostly in pieces published in The Atlantic and The New York Times.
And importantly, I’m far from the only one to hold this view.
Is it her diverse educational and vocational background? The fact that she’s a true “citizen of the world,” having lived in multiple places? That she works really, really hard to get things right? That’s she’s also wicked smart, to coin the Bostonian phrase to describe the smartest person in the room?
Probably all of the above.
Zeynep kindly joined me recently on this Open Forum Infectious Diseases podcast to discuss how she ended up in her interesting current position, and her approach to COVID-19 — how we missed the mark for well over a month on the seriousness of the problem, our missteps on masks, the continued penchant for “beach scolding,” how we undersell the vaccines, and the general timidity of the biomedical community in questioning authority.
And yes, she finishes by speculating how this might end.
Highly recommended.
Transcript here. Also available on Spotify, Apple Podcasts, etc.
March 14th, 2021
Really Rapid Review — CROI 2021 Virtual
 For a few years in the early 2010s, the Conference on Retroviruses and Opportunistic Infections (CROI) — in my opinion our premiere HIV scientific meeting — covered almost as many hepatitis C clinical trials as those on HIV. Or at least it seemed that way.
For a few years in the early 2010s, the Conference on Retroviruses and Opportunistic Infections (CROI) — in my opinion our premiere HIV scientific meeting — covered almost as many hepatitis C clinical trials as those on HIV. Or at least it seemed that way.
This made sense at the time — the startling success of non-interferon-based HCV treatments made for exciting news, and rapid progress. Here’s what I wrote in 2013 in another patented, copyrighted, and trademarked CROI Really Rapid Review™, for which NEJM Journal Watch receives many millions of dollars in royalties:
The results of the sofosbuvir and ledipasvir study — 100% response in both naives and prior null responders — provided one of the more exciting clinical trial results I’ve seen in years, small sample size notwithstanding.
Remember those days? Well, this CROI had barely any HCV at all, a sign of progress.
(And I was kidding about the royalties, in case you were wondering.)
Of course, in 2021 we are in the midst of a pandemic, so it’s not surprising that this CROI had plenty of COVID-19 studies, both on COVID-19 alone and on the combination of HIV and COVID-19. Here are some highlights, starting with HIV, then the HIV/COVID-19 studies, and then some interesting COVID-19 alone papers.
The links are to the presented abstracts, which requires a conference account (at least it does today) — however, as with other HIV meetings, plenty of the presented material appears on the invaluable NATAP page.
- In the NADIA study, second-line therapy with dolutegravir was non-inferior to darunavir-ritonavir, and tenofovir/FTC non-inferior to ZDV/3TC. This beautifully done randomized clinical trial included patients with extensive NRTI resistance — lots of K65R plus M184V. Though conducted in Africa, it has lessons for us all, including: 1) residual activity of NRTIs even with high-level resistance; 2) imprecision of consensus interpretations of genotype tests, 3) no need for ZDV in those with K65R (phew), and 4) the need to monitor for INSTI resistance — even though it’s rare (just 4 cases out of 235 randomized to DTG), it has major clinical implications.
- In a large, US-based clinical cohort of people with advanced HIV disease, BIC/FTC/TAF was the three-drug regimen least likely to be discontinued. Also, a higher proportion had viral suppression than on boosted darunavir. These two strategies are being directly compared in the ongoing LAPTOP study in this very population. Speaking of people with advanced HIV disease …
- A cohort of 912 patients starting ART with various regimens favored initial integrase-based treatment over regimens with NNRTIs or PIs. Benefits were lower discontinuation rates and mortality. And more on this population …
- In a small (n=101) randomized trial in people with CD4 < 100, ABC/3TC/DTG had fewer drug discontinuations than ABC/3TC plus darunavir/ritonavir. Bacterial translocation was also lower with the DTG-based regimen. Note that higher rates of discontinuation of PI-based regimens have been observed before in patients with advanced disease. Speaking of this DTG versus DRV comparison …
- In an open-label randomized trial (n=306) in treatment-naive patients, DRV/c/FTC/TAF did not meet non-inferiority versus ABC/3TC/DTG. In other words, it was not noninferior — now you can show off to your statistician friends by using that double-negative language. Notably, weight gain was a bit more with DRV than DTG. (Shrugs.)
- In treatment-naive studies of BIC/FTC/TAF and DTG plus either TAF/FTC or ABC/3TC, viral suppression was still very high, even with transmitted drug resistance. The investigators used retrospective baseline next-generation sequencing of PR, RT, and integrase, with a 15% cutoff. Importantly, pre-study standard genotyping that identified resistance to the NRTIs was exclusionary.
- Injectable cabotegravir and rilpivirine given every 8 weeks remains non-inferior to injections every 4 weeks at week 96. The current approval in the U.S. is for the 4-week strategy; approval of the 8-week approach is expected soon.
- For those switching to DTG/3TC, having M184V detected more recently increased the risk of virologic failure. This was compared to those with no historical M184V, and those in whom it had been found more than 5 years previously. Of course, this begs the question — why switch to DTG/3TC with a known M184V? Despite the ongoing activity of 3TC, this is not how the DTG/3TC regimen was studied. I wouldn’t do it.
- In a clinical cohort, predictors of 10% or more weight gain after switching to integrase-based ART were being female, underweight/normal weight, prior non-INSTI treatment, and the TDF to TAF switch. There was no difference between different INSTIs, however.
- Integrase-based ART was associated with an excess risk of cardiovascular events — but only after the first 6 months of exposure. It’s an observational study, so we cannot determine causality (just as we couldn’t with the first abacavir CVD study). And how do we explain that the effect was only temporary?
- In a database analysis of over 34,000 people starting or switching to integrase-based ART, new-onset diabetes or hyperglycemia occurred in 2.5%. This was significantly higher than non-integrase-based ART, with dolutegravir carrying the highest risk. Bictegravir was not included (database stopped in 2018), and there was very little TAF use.
- For pregnant women starting ART during pregnancy, DTG + TAF/FTC, DTG + TDF/FTC, and EFV/TDF/FTC had comparable viral suppression at 50 weeks’ postpartum. Pregnancy outcomes favored the TAF arm of the study — will our guidelines be updated soon based on this trial?
- In that study, the women in the DTG + TAF/FTC arm gained the most weight. However, this weight gain was closest to the recommended weight gain during pregnancy and also associated with a lower risk for any adverse pregnancy outcome, suggesting that pregnant women treated with EFV/TDF/FTC don’t gain enough weight.
- When started late in pregnancy, dolutegravir achieved viral suppression more rapidly than EFV. In this randomized trial of 237 women, there were three in utero HIV transmissions in the DTG arm, and one post-partum transmission in the EFV arm.
- A 4-month daily regimen of rifapentine and moxifloxacin was noninferior to the standard 6-month regimen for tuberculosis treatment. The participants also received isoniazid and pyrazinamide for the first 8 weeks. Anything that shortens TB treatment is a real advance!
- In highly treatment-experienced patients, oral lenacapavir induced a 1.93 log viral load decline (vs. 0.29 in placebo) after 14 days when added to a failing regimen. At this point, treated patients switched to subcutaneous lenacapavir given every 6 months, along with an optimized background regimen. The study is ongoing (and includes a non-randomized arm), and 19/26 patients have viral suppression. Two experienced viral rebound with emergent resistance. Not much information about the background regimens used with this novel agent.
- The investigational NNRTI MK-8507 has a PK profile that supports once-weekly dosing. It will be paired with islatravir for treatment of HIV. The resistance profile is likely to be similar to doravirine.
- Further evaluation of daily versus on-demand PrEP with TDF/FTC shows a low incidence of HIV in both strategies. One wonders whether TAF/FTC would be this effective given on-demand — suspect it would be, but it has not been tested this way.
- Laboratory evaluation of cabotegravir PrEP failures in HPTN 083 was challenging. And that’s an understatement! The issue is that CAB delayed detection of infection using standard HIV testing algorithms (point-of-care antibody testing, standard 4th generation antigen/antibody tests). Also, a small number failed despite adequate adherence and measured CAB levels, with development of INSTI resistance. Should we be using viral load tests to monitor our patients on CAB-based PrEP? Likely yes.
- A cost-effectiveness analysis of long-acting CAB for PrEP suggested that it would not be cost-effective if priced similarly to cabotegravir-rilpivirine. Though CAB is more effective than generic TDF/FTC for HIV prevention, the estimated $17,000/year cost difference puts the cost-effectiveness ratio at more than $1 million per quality-adjusted life-year. A limitation of this analysis, of course, is that we don’t know yet what CAB for PrEP will cost!
- As both a pill and as a drug-eluting implant, islatravir moves forward as a long-acting PrEP option. The pill projects to be once-monthly; the implant could be yearly.
- In consecutive sampling of 1076 people with HIV (PWH) in Spain, 8.6% were seropositive for SARS-CoV-2. Those on TDF/FTC were less likely to test positive — even after controlling for underlying comorbidities (an adjustment not made in this group’s previously published paper).
- In a large national cohort with nearly 600,000 cases of COVID-19, PWH and solid organ transplant recipients were more likely to be hospitalized than controls. Both groups had a high burden of comorbidities — which increases the risk of adverse outcomes from COVID-19 for all groups, including those with HIV.
- A single infusion of bamlanivimab and etesevimab given to outpatients with COVID-19 at high risk for severe disease reduced the risk of clinical progression (hospitalization or death). There were no deaths in the treatment arm, 10 in placebo. Viral load decline and clinical recovery were also faster with treatment.
- Compared to placebo, the oral antiviral molnupiravir reduced the proportion of patients who had positive SARS-CoV-2 viral cultures by day 5. Unusual endpoint, but the results do demonstrate an antiviral effect. Several phase 3 clinical trials are ongoing, both in the inpatient and outpatient setting.
- Banlanivimab was effective in preventing COVID-19 in skilled nursing facilities. Those who did get COVID-19 despite treatment had lower viral loads and more rapid resolution of symptoms compared to the placebo group. While vaccination will undoubtedly be the mainstay of preventive strategies for COVID-19, in certain settings monoclonal antibodies may have a role.
- In another study of COVID-19 prevention, casirivimab plus imdevimab given subcutaneously to asymptomatic household contacts of active cases prevented 100% of symptomatic infections. Among those who did acquire COVID-19, viral loads were lower and PCR positivity was of shorter duration compared to placebo. Note the subcutaneous route of administration in this study, as it obviated the need for IV access — a big advance given the difficulty of arranging these treatments under the current Emergency Use Authorization.
- For 23 patients with refractory COVID-19 due to B-cell deficiency, convalescent plasma led to clinical recovery in 20. This population — receiving rituximab or similar anti-CD20 agents — has proven particularly vulnerable to COVID-19, often with prolonged symptoms and persistently high levels of virus.
- Treatment of hepatitis C with sofosbuvir/velpatasvir achieved cure in 95% of patients with minimal monitoring. And I mean minimal! (The study was called “MINMON”.) This single-arm study with 399 participants dispensed all tablets for a 12-week course at entry, had no on-treatment laboratory monitoring, and had just one week 22 visit to assess for cure (SVR). Aside from two phone contacts for adherence monitoring, that was it — amazing.
- Didn’t see all the plenaries or invited talks — attending a virtual conference can be strangely exhausting — but among those I did see, can highly recommend Dr. Shahin Lockman on HIV treatment in pregnancy, Dr. Jose Arribas on dual versus triple ART, and Linda-Gail Bekker on long-acting options for HIV prevention. Bravo!
You’ll note I started and finished this post mentioning hepatitis C studies — which due to our success in treatment now have a very small footprint at CROI. Let’s hope the same happens to COVID-19 in the not-so-distant future!
And since this CROI was supposed to be Chicago and bring in people from all over the country (and the world), here’s a wonderful tour around North American accents, with of course a stop in the land of da Bears — right around 3’40”.
March 7th, 2021
Exactly One Year Ago, a Memorable Dinner Before a Memorable Year
Feb 23, 2020.
On March 7, 2020, right before CROI here in Boston, a bunch of us ID types planned to get together for a pre-conference dinner. A mixture of Bostonians and out-of-towners who hadn’t seen each other for a while. A chance to catch up before our busiest (and most important) scientific meeting.
What happened?
One person landed in Boston, and promptly got the next flight back to Los Angeles.
Another canceled his flight and never left home. A shame, too, since he was bringing his new partner (whom I still haven’t met). I hear she’s really fun and interesting.
One had to stay home due to a no-travel ruling issued for all his faculty. (Those edicts had not yet come from Harvard, but would a week later.)
A fourth had arrived early for the conference, but was so busy setting up the now “virtual” CROI that dinner for her was out of the question.
And of course, attendees from Europe (especially) already had pulled out of the conference en masse.
You get the idea.
Our numbers for dinner were substantially down, but we still assembled with (mostly) locals. Indoors. Windows closed. It’s winter here in early March. Plenty of hand-washing and, befitting the fomite-centric perspective at the time about SARS-CoV-2 transmission, extra use of an alcohol-based hand sanitizer — something I’d never purchased before.
That evening was filled with lots of discussion about the Biogen conference. About China, Italy, Spain, and Iran, and what was undoubtedly coming our way soon. About our frustration with the lack of COVID-19 testing — we ID doctors spent all of February complaining about that, with no answers coming from anywhere. Just painful silence.
And, yes, lots of anxiety.
Now, as CROI starts up again — virtually, of course — I think back to that night. A dinner indoors with friends and colleagues, possible a year ago today but unimaginable since, could now again happen in our (fully vaccinated) future.
Not saying I know when it will happen — just that it could. Hope.
Wow, it’s been a memorable year.
February 28th, 2021
Another COVID-19 Vaccine — and Barney, Explained
 Busy few days on the COVID-19 vaccine front, specifically related to the Ad26.COV2.S vaccine developed by Johnson & Johnson.
Busy few days on the COVID-19 vaccine front, specifically related to the Ad26.COV2.S vaccine developed by Johnson & Johnson.
February 26, the Vaccines and Related Biological Products Advisory Committee reviewed the data on the vaccine, voting unanimously that the benefits outweighed the risks.
February 27, the FDA granted the single-dose vaccine emergency use authorization.
And February 28-March 1, the Advisory Committee on Immunization Practices (ACIP) meets to discuss what recommendations to make about its use.
This means doses can reach us as early as this week.
What is this vaccine? Ad26.COV2.S is a recombinant replication-incompetent human adenovirus serotype 26 vector encoding a full-length, stabilized SARS-CoV-2 spike protein antigen.
In other words, quite different from the mRNA vaccines in current use, and hence requiring a whole new section to the NEJM Covid-19 Vaccine Frequently Asked Questions.
That’s a ton of work (for me), which is why this week’s post is so short.
But before I go, here’s the inspiration for citing an anthropomorphic dinosaur as my “animal spirit”, as requested by Dr. Gabriel Vilchez:
— Paul Sax (@PaulSaxMD) February 27, 2021
My friend Janet — a brilliant child psychiatrist — used to tell her pre-teen daughter why she couldn’t get a tattoo.
The reason?
Imagine if I had let you get a tattoo when you were 4 years old. You’d have Barney the Dinosaur on your body permanently. Who knows whether what you love now will be something you will love the rest of your life.
This was a highly effective message, one I’ll never forget.

Paul E. Sax, MD
Contributing Editor
NEJM Journal Watch
Infectious Diseases
Biography | Disclosures | Summaries
Learn more about HIV and ID Observations.