
An ongoing dialogue on HIV/AIDS, infectious diseases,
December 10th, 2017
Injection Drug Use-Related HIV Cases Increase in Massachusetts — Is This the Start of a Trend?
Recently the Massachusetts Department of Public Health sent out this concerning notice:
The Massachusetts Department of Public Health (MDPH) has noted an increase in newly diagnosed and acute HIV infections among persons who inject drugs (PWID). To date in calendar year 2017 (through November 21), there have been 64 HIV infections reported among individuals who inject drugs in Massachusetts … Over the past 5-10 years, newly diagnosed HIV infection in PWID amounted to 32-62 cases annually, representing a stable proportion of 4-8% of all reported HIV infections. Investigation of cases is ongoing.
Undoubtedly, one reason for the notice is that it stands in stark contrast to a long-term trend. Indeed, the drop in injection drug use-related HIV has been one of the unheralded success stories in the USA HIV epidemic.
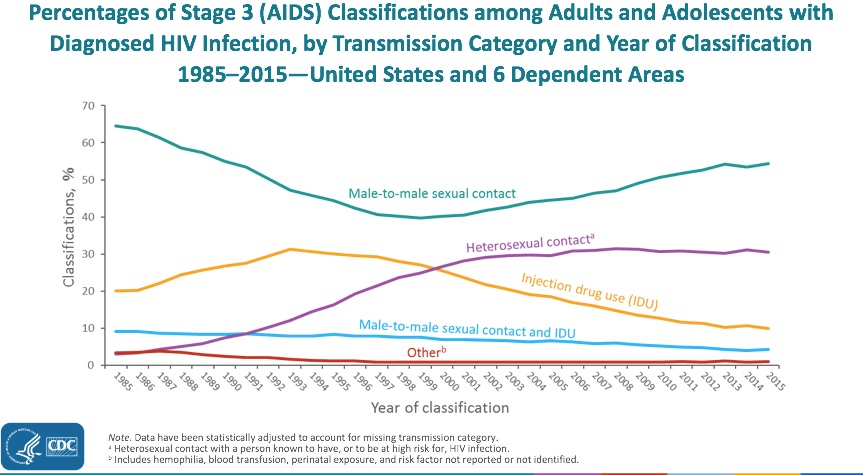
Once a very prominent “transmission category,” it has declined more than any other risk factor, now accounting for less than 10% of new HIV diagnoses per year. For a broader view, here are AIDS cases in the USA since the beginning of the epidemic, showing the steady decline in cases attributable to injection drug use since the mid-1990s:
This decrease in cases is even more remarkable when viewed in the context of our national opioid epidemic, a problem we ID doctors are reminded of on a daily basis — not from HIV, but from serious invasive bacterial infections and, to a lesser extent, hepatitis C.
By contrast, new cases of HIV due to injection drug use alone are now relatively uncommon in the United States. A notable recent exception was the 2015 Indiana HIV outbreak, where nearly 200 new HIV infections occurred in four months in a rural community hard-hit by opioid addiction.
A skillful CDC investigation found that just one person with HIV was the source of the outbreak, which was then fueled by a needle-sharing network. The outbreak demonstrated the potential rapid spread of HIV in this population — and then the ability of syringe exchange programs to control it.
Are we seeing the beginning of something like the Indiana outbreak now in Massachusetts? Or is this year’s increase — admittedly rather small to date — just a temporary blip?
Regardless, good work by the MDPH in getting the word out — vastly preferable to be early rather than late to recognize this trend.
I’ve heard anecdotally there might be other HIV outbreaks nationally among people who inject drugs. What’s been your experience where you practice?
6 Responses to “Injection Drug Use-Related HIV Cases Increase in Massachusetts — Is This the Start of a Trend?”

Paul E. Sax, MD
Contributing Editor
NEJM Journal Watch
Infectious Diseases
Biography | Disclosures | Summaries
Learn more about HIV and ID Observations.
While I’m not seeing more cases of hiv, I’m seeing more undiagnosed hcv in patients coming to my office for opioid use disorder. Many of these people have been to substance use clinics and not screened, that’s not where their money is.
HCV is prevalent among drug users. PWID have local transmission networks and viral transmission depends greatly on the prevalence. In the case of HIV infection, the prevalence is lower than for HCV and most of them are on therapy.
If we take into account the current opioid epidemic in the US and if in the coming years harm reduction strategies and therapy are not implemented in this population group, HIV incidence and prevalence will sharply rise in the next decade.
I’ll be sure to tell my colleague, who was the chief investigator for the Indiana outbreak, that you called his work skillful.
When I worked in the Tenderloin, we had a lot of IVDU patients as we were on skid row. We quietly supplied clean needles in our clinic, and taught pts how to inject safely.
When I got to my current, more middle-class, corporate-ish environment, I was shocked at the lack of IVDU pts. Like I can think of maybe 2 on my caseload of 380. I was sad, as I am a recovering heroin user myself, and I was eager to help out some of “my people.” It sounds like now transmission is breaking class lines in MA, so maybe this too will cause some change at a state level (like it did in Indiana).
Thanks for bringing up this topic.
Your loyal NP,
D
Oh, I also wanted to mention that more people than ever are jumping straight to heroin; the stereotype of the over-medicated patient advancing to heroin is not happening as often.
In this study, a cohort of opiate users in treatment were polled. In 2005, 8.7% of opiate addicts had jumped straight to heroin. In 2015, 33% had jumped straight to heroin.
With people all over this country seeking relief from the distress of modern life, and the ridiculous availability of Mexican heroin, and with the black market for pills now being sky high ($2/mg for oxy), we are in serious trouble. The deaths keep climbing.
Suboxone saved my life, and it still does. Please get your X number and help your patients who need it.
Dangit, the aforementioned study is:
https://www.ncbi.nlm.nih.gov/pubmed/28582659/
Working in Baltimore, you can guess the effect of IVDU on HIV and HCV transmission, and while we had a nice downwards trend until just last year when the opioid epidemic decided to kick it back up a notch. It’s still not as big as sexual transmission by gross count, but, uh, it wouldn’t be amiss for me to state my feeling that the rate of frequency of sexual encounters in the metropolitan area compared to the rate of injection drug use wouldn’t be a specious comparison. We do have that much usage, sadly.
Source:
https://phpa.health.maryland.gov/OIDEOR/CHSE/Pages/statistics.aspx