
An ongoing dialogue on HIV/AIDS, infectious diseases,
November 18th, 2018
HIV and HCV Treatment, Shorter Antibiotic Courses, Malaria-Sniffing Dogs, and Other ID and HIV Reasons to Be Grateful, 2018 Edition
As noted here before, I’m a big fan of Thanksgiving, a great excuse to get together with family and friends, and to eat a gargantuan amount of food.*
(*On this last point, non-U.S. citizens will wonder how this differs from any other time we “Americans” get together. Indeed, we are the Land of Giant Portions. Ever eat at a Cheesecake Factory? Yeesh.)
But the primary purpose of Thanksgiving is expressing gratitude, a very healthy impulse that makes everyone happier. And since this is an ID blog, here are bunch of things ID and HIV specialists can be thankful for over the past year:
- HIV treatment continues to improve. In the past year, we’ve seen approvals of bictegravir/FTC/TAF, darunavir/c/FTC/TAF, doravirine and doravirine/3TC/TDF, and ibalizumab. If that’s not enough, generic 3TC/TDF and EFV/3TC/TDF also gained FDA approval. Treatment now is so good with bictegravir and dolutegravir-based regimens that essentially 100% of patients taking these simple, well-tolerated regimens achieve viral suppression, and the IAS-USA Guidelines responded by making them the preferred treatments. Starting HIV treatment on the same day of diagnosis has moved from an interesting idea to a practical reality (especially with bictegravir/FTC/TAF and darunavir/c/FTC/TAF). Finally, the remarkably good results of the two-drug dolutegravir plus 3TC regimen in the GEMINI studies suggest that therapy can be even safer — and cheaper — than it is now.
- When it comes to the duration of antibiotic therapy, less is almost always better than more. A barrage of studies have shown that almost regardless of the condition, a shorter course of antibiotic treatment is the right choice. Shorter is better than longer both in the hospital and in the outpatient office. The take-home message from these data should be that clinicians can use their clinical judgment to decide how long to treat someone, not relying on some arbitrarily chosen treatment course — and yes, I mean even a treatment course defined by an ID doctor.
- It is becoming increasingly clear that oral antibiotics can substitute for intravenous in almost every situation. In the much-discussed POET study, stable patients with endocarditis who completed treatment with oral therapy did just as well as those who completed treatment with IVs. (And here’s a big thank you to Dr. Grace Farris for allowing us to use her wonderful journal club cartoon.) In another study, linezolid — price dropping rapidly — was a fine option for completing treatment in uncomplicated Staph aureus bacteremia. OVIVA study, where are you?
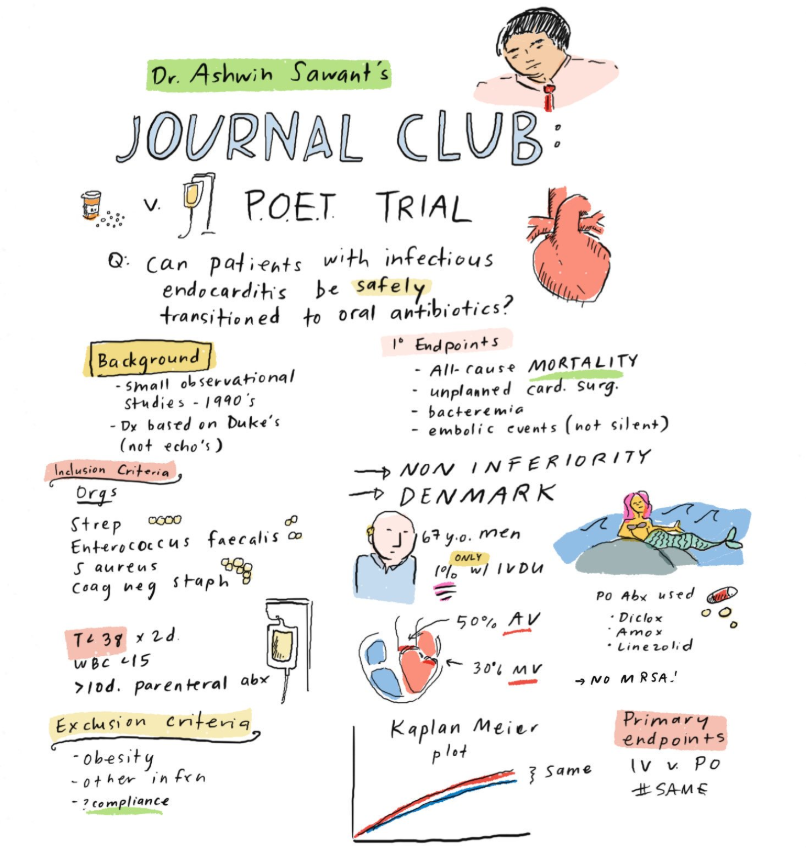
POET Study, by Grace Farris, MD (click to enlarge).
- Hepatitis C treatment has become staggeringly simple. I’m going to estimate that 99.156% (approximately) of treatment-naive patients could be successfully treated with either 1) sofosbuvir/velpatasvir, one pill daily for 12 weeks or, 2) glecaprevir/pibrentasvir, three pills daily for 8 weeks (sometimes 12). Go ahead and abbreviate SOF/VEL and GLE/PIB, if you find saying them a mouthful. Both are pan-genotypic, safe, well tolerated, and incredibly effective, and the price has dropped dramatically since the crazy days of 2014. In other words, these are the “must know” HCV treatments; the rest are optional. Here are a couple of slides I’ve made to describe a few of the medical issues in the choice between them — it’s a very short lecture — since most of the time, either one will do.
- Undetectable = Untransmittable, even in the highest-risk patients. The first publication of the PARTNER study of “condomless sex” among HIV serodiscordant couples didn’t have enough MSM couples to make a confident statement about the risk in this population. No longer — in a follow-up presentation this summer in Amsterdam, 783 MSM couples contributed data including 1596 couple-years of follow-up, and 76,991 (impressive precision!) condomless sexual encounters — and there were still zero transmissions. Giving this U=U message to our patients never gets old.
- Treatment of African trypanosomiasis will very soon be safer, easier, and more effective. Current treatment for this life-threatening parasitic infection — better known as “African sleeping sickness” — involves a complicated infusions with the drug eflornithine (administered in a hospital) along with nifurtimox. By contrast, fexinidazole (just approved) is given as one pill daily for 10 days and is both more effective and less toxic. Thanks to several European countries, the Bill and Melinda Gates Foundation, Doctors Without Borders, and other donors for funding the study that led to its approval, which was coordinated by the Drugs for Neglected Diseases Initiative.
- Preventive therapy for latent TB is getting shorter. In a large randomized study, a 4-month rifampin regimen was just as effective as 9 months of INH, and was both less toxic and more likely to be completed. In people with HIV, 1 month of daily rifapentine/INH prevented TB as well as 9 months of daily INH. The latter study hasn’t yet been published — and included some “high risk” patients who lacked positive skin testing or IGRA studies — but one is hopeful that the favorable results would translate to people without HIV as well.
- There continue to be ID-related studies that test the diagnostic skills of dogs. I guess they can’t reliably sniff out C. diff after all, but they did pretty well identifying malaria from the socks of children. (Yes, that’s what they were asked to do. Dogs will sniff anything.) I don’t actually think any of these dog diagnostic strategies will ever become standard-of-care (alas), but the videos and pictures released with each study sure are cute.
What are you grateful for this Thanksgiving?
2 Responses to “HIV and HCV Treatment, Shorter Antibiotic Courses, Malaria-Sniffing Dogs, and Other ID and HIV Reasons to Be Grateful, 2018 Edition”

Paul E. Sax, MD
Contributing Editor
NEJM Journal Watch
Infectious Diseases
Biography | Disclosures | Summaries
Learn more about HIV and ID Observations.
 NEJM Journal Watch — Recent Infectious Disease Articles
NEJM Journal Watch — Recent Infectious Disease Articles- Observations from ID and Beyond: Federal HIV Guidelines Face a Shutdown — A Critical Loss for Clinicians and Patients
- Ceftriaxone for Patients Hospitalized with Pneumonia: One Gram or Two?
- More PrEP, Less HIV: U.S. State Data
- Observations from ID and Beyond: Why the Sudden Firing of ACIP Members Should Put Every Clinician on High Alert
- Does HIV RNA Testing to Monitor PrEP Add Value?
great ID 2018 highlights
One of those articles that makes you realize how interesting ID is, and makes you fall in love with ID again! Thank you, Dr. Sax.