
An ongoing dialogue on HIV/AIDS, infectious diseases,
July 5th, 2020
Rapid, Inexpensive Home Testing for COVID-19 May Get Us Out of This Mess Before a Vaccine
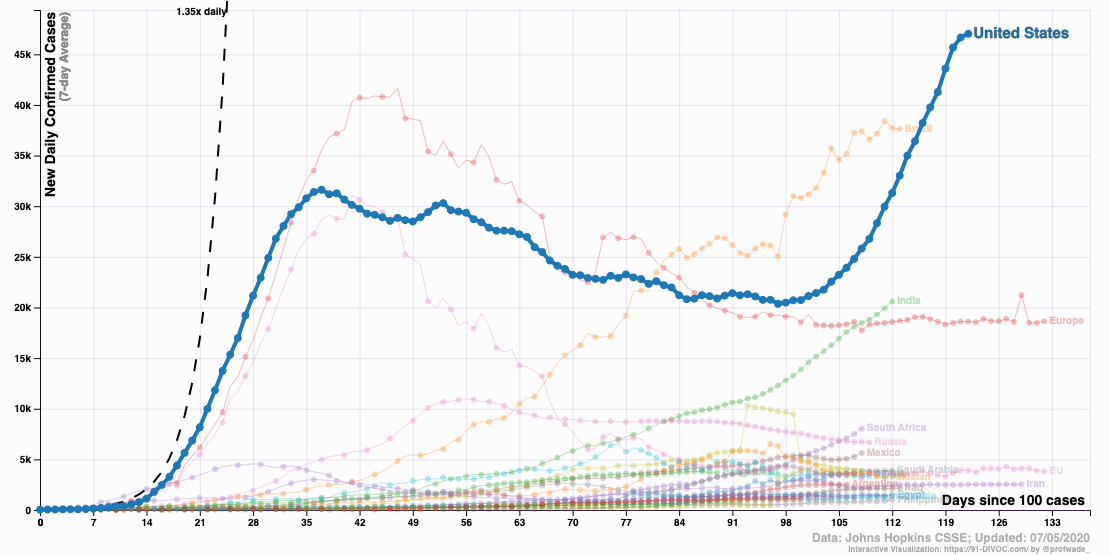
Source: 91-divoc.com/pages/covid-visualization/
As cases of COVID-19 continue to climb to record numbers, it might seem impossible that something is already out there that could dramatically reduce new infections — and even bring us back to some semblance of normal life.
I’m not referring to a vaccine. It’s a rapid, inexpensive home test.
You’re forgiven for being incredulous. Indeed, you might be discouraged by a depressing sense of deja vu as you hear that hard-hit communities again must suffer delays on both obtaining tests and getting results.
And it’s not just Arizona, Texas, and Florida. Testing volume for COVID-19 has so overwhelmed commercial and national reference labs that turnaround times to get results are at the very least several days, and can be a week or longer — tests ordered from anywhere in the country.
Didn’t we learn anything from our lack of tests in the winter and spring, when contagious cases went undetected because of our inability to test all but symptomatic people? Didn’t that allow those with mild or pre-symptomatic disease to continue to spread the virus in the community, triggering an explosive increase in cases?
The problem is that we’re doing it all wrong. Again.
We need to test more broadly, even in people without symptoms. The critical window period for transmitting the virus starts a day before symptom onset.
And instead of relying on the gold standard for diagnosis — the polymerase chain reaction (PCR) tests, done on a nasopharyngeal swab — we need to lower the bar for accuracy and use one of the many rapid tests currently in development.
As noted in this spot-on perspective on rapid home tests written by Drs. Laurence Kotlikoff and Michael Mina, our PCR testing, while accurate, has many problems — it’s expensive, it’s slow, and it strains the lab supply chain. Our hospital has had to diversify the PCR tests it offers to at least 5 different platforms to avoid running low on any one particular test.
Some might argue PCR is too sensitive — it picks up fragments of viral RNA long after a patient is no longer contagious. These positive results generate all kinds of confusion and worry.
In addition, a nasopharyngeal swab requires trained personnel to obtain the sample. It hurts, too, as anyone who has had the test will tell you. There’s a reason the most common “joke” heard after undergoing PCR testing is likening it to a pituitary biopsy. Ha ha.
So why don’t we have rapid, cheap home tests available now?
It’s not for lack of trying — take a look at this list of companies working on the problem as of early June:
Thanks, Tomas
That makes 16 pic.twitter.com/QQcBDopaGL— Eric Topol (@EricTopol) June 7, 2020
Apparently, one thing that may be holding up FDA approval of these tests is that they are less sensitive than the PCR. That means they’re more likely than the PCR to miss someone who has COVID-19, wrongly giving a sense of reassurance from a false-negative result.
This is a legitimate concern, but one that should not block their urgent approval anyway. We should welcome these tests, even if less accurate, and broadly adopt them for widespread community use. Here’s why:
- They will be cheap. Estimates are that they would cost between 1 and 5 dollars. That’s around the price of a cup of coffee.
- They can be done on saliva. No brain biopsy required.
- They can be done frequently. Every day for college students, or healthcare workers, or bus drivers? Every third day for everyone?
- They will answer the key question — am I contagious to others right now?
Finally, and most importantly, they will answer this last question quickly. Results back in less than an hour.
Anyone with a positive test can self-isolate, be reported to public health officials, participate in a contact tracing program, and be monitored for symptoms. Maybe pre-emptive antiviral therapy will prevent severe illness.
We can choose to do a rapid home test any day we go to work, or to the gym, or to meet friends in a restaurant, or to attend a concert, or to pray in a house of worship, or to visit an elder loved one, or indeed partake in any activity we do in groups that now sadly may sustain the pandemic.
And for those worried about lack of sensitivity, two items of reassurance. First, false negatives are less likely when people have the highest amounts of virus in saliva and respiratory secretions — and this is when they’re most contagious to others. If the test is falsely negative due to low titers of virus, it may not matter very much.
Second, this modeling study finds that the frequency of testing is the key determinant of how well a broad testing strategy will limit the spread of the virus. It’s even more important than test sensitivity, and evidence that imperfect testing is better than no testing at all.
So bring on the rapid home tests — lower sensitivity notwithstanding — and the sooner, the better.
It’s one thing that could make Olive and Mabel’s retirement easier to take. Maybe they’ll even do a reunion tour.
72 Responses to “Rapid, Inexpensive Home Testing for COVID-19 May Get Us Out of This Mess Before a Vaccine”

Paul E. Sax, MD
Contributing Editor
NEJM Journal Watch
Infectious Diseases
Biography | Disclosures | Summaries
Learn more about HIV and ID Observations.
 NEJM Journal Watch — Recent Infectious Disease Articles
NEJM Journal Watch — Recent Infectious Disease Articles- Is Cardiovascular Risk Sustained After SARS-CoV-2 Infection?
- Which Hepatitis B Vaccine Provides the Longest-Lasting Protection in People with HIV?
- Lenacapavir for HIV Preexposure Prophylaxis: Guidance from the IAS–USA
- Is All-Oral Treatment an Option for Whipple's Disease?
- Two Doses of Recombinant Zoster Vaccine Worked Well in People 50 and Older
Brain biopsy – that’s it exactly.
haha, or to “woman-splain”: a pap smear
I am not sure if we are talking about antigen rapid test or antibodies. Unfortunately, antigens have low sensitivity. And antibodies, although have better sensitivity, they are positive about 1-3 weeks after symptoms onset, limiting the efficacy in reducing the transmission, as the higher period of transmission is about 1-2 days before up to 7 days after symptoms onset.
However, it could be a good tool for retrospective diagnosis.
Reunion tour? What would you call it? Dog eats dog? Spot on comments paul. Let’s choose frequent home tests with less sensitivity but with consecutive and frequent testing more functional value. The pcr tests just take too long to be if real value in day to day decisions
Paul, you have too much faith in your fellow humans. Many people will take the test, see that they’re infected and, unless they are very ill, will go about their day infecting those around them. It’s evident that the public is more concerned with having a good time and returning to “normal” than being ethical and caring about anyone else otherwise mask wearing and social distancing would be the norm. There are parties being held by teenagers to intentional infect others. This can’t be fixed by anything except Darwinism.
I loved Nancy Rosen’s comment. Sad, but so true. Exactly why we can never fix our soaring health care costs. You and my son are on the same page with Darwinism….
Seems anyone with such
lack of concern for others wouldn’t bother to pay the money or rake the test.
the majority of Americans think we are reopening too quickly
https://s.abcnews.com/images/US/IpsosPoll_Coronavirus_Q2_QuickSlowRightPace_070920_v01_KS_hpEmbed_16x9_992.jpg
Thanks,
This seems like a good avenue to explore.
However as we have low population prevalence of the disease in the order of 5-15 percent based on antibody studies a test with low sensitivity will likely result in low PPVs. What is the PPV that would be considered acceptable?
The antigen tests should have a much higher specificity than antibody tests.
Thank you for your excellent and sane voice.
Perhaps Olive and Mabel can be trained to “sniff out” infected folk?
Again our lovely FDA working against us. Are they doing any at home testing in other countries? If so, wouldn’t that be a resource for the USA?
Test, Trace, Isolate and Support. Rapid testing is much more sensitive than NO testing. Test often and make available to all!
This is really the comparison to make – not some gold standard, but what is the population impact of a “worse” test being done on more people and more often – compared to nothing.
Great point. How about we add “educate” to this approach:
(1) Educate
(2) Test
(3) Trace
(4) Isolate
(5) Support
We can learn from other countries—what they did right and what they did wrong. Testing and contact tracing is key, and yet it’s so complicated to get a test and get the results.
I think we may be oversimplifying several issues.
We know that many patients will not have the desired response to a positive test, or will misinterpret a negative result after exposure. This may be a major challenge, but it is not as simple as lack of concern for others. How many physicians are not guilty of “presenteeism?” And many of our COVID patients have low-paying jobs with no paid sick leave. I keep hearing, “How hard is it to stay home and watch Netflix?” It can be very hard if you don’t have any money, and our country has spent the last 3 decades hacking away at the safety net.
The relevant comparator for a home test is not an in-lab test or no test at all, it is a complicated mixture of both. Analyses that assume a home test will replace only one or the other of the alternatives will be interesting but may not produce accurate answers for the real world. But it is as hard to predict what people will do for testing as it is to predict what they’ll do with their results, and it will very greatly depending on the patient’s situation. In other words, it should be studied. Like much of the COVID endeavor, it will probably be studied in real-world use rather than before release.
Finally, home test results will not be reported to Public Health, and that may have a significant effect on contact tracing and our ability to understand the burden of disease in the community.
Home tests could be bluetooth-linked to a smart-phone app that automatically reports positives. The “Kinsa” thermometer does fever reporting anonymously and has been an excellent early sentinel for influenza and CoVID 19 (early on); although there are privacy concerns, and I am a privacy nut, I would be willing to REPEATEDLY purchase a home detection kit with automated reporting.
I absolutely agree with Dr. Sax that frequent testing, of potentially the population, but at a minimum “essential workers”, is the best course currently available to stem the tide.
It would also a nice touch if companies who asked that employees STAY HOME ON PAID LEAVE while sick until they have a CoVID 19 test done, could then submit the expense for federal “paycheck protection” money..
What a sane and practical idea. Maybe when the Senate and our fearful leaders get around to the next covid bill, they will put this in.
Hope is thin gruel, but sadly it is all we’ve got.
I mostly agree with Dr. Sax’s analysis. In the balance, there will probably be more benefit than harm. The test performance could be enhanced if combined with virtual care, ideally with a trained professional, but even an AI medical chatbot could be helpful for addressing situations like a recent covid-19 exposure. Some employers might pay to provide their employees with testing, especially if it included automatic reporting of tests in order to reassure their customers and the rest of their workforce.
Anything that will get more people tested is good.. I agree with many of the comments – irresponsible communities and individuals has made this an overwhelming public health concern. I work one of the hospitals impacted by COVID in Houston TX . It is non-stop admissions and our hospitals in the med center are accommodating the cases. The other issues include the fact that other people are still sick still need our care and by the time they -the compliant patients – arrive to the ER they are critically ill. Downtime spent screening them often delays care. A rapid test home based works for me. And fingers crossed a vaccine soon.
What do you folks think about a having/using a hyper-intelligent mobile app that would let people every day:
(1) perform a “self symptom assessment” and high risk medical history screening
(2) provide each person the best actions to take based on their results and what’s happening in the area where they live (e.g. isolate, get tested, see a doctor, go to emergency room, etc.)
The bottom line is the United States was and continues to be unprepared to handle such a crisis. Crimson Contagion for example.
1000 Healthcare workers have died from this at this time.
We have a compromised health care system.
“All this nonsense has to stop we have a serious public health crisis”
— Dr. Peter Hotez
Home testing seems like a no brainer, especially using the KISS method.. The accuracy of the nasal swap testing isn’t anywhere near 100% let alone the discomfort factor. U of Illinois is doing it.
Yes i agree,that we must to use all possibility for the early detection of COVİD 19.First of all,tests should be done in healthcare workers.Deaths among medicals,i think,determined by repeated infection. More and more virus loading in healthcare worker before they became symptomatic makes disease severe and impact survival.Therefore tests,absolutely,nessecary,everyday tests in this cohort.Also,in hospitals,where tests for the coronavirus PCR or immediate is unavailable or limited,it is possible to obtain laboratory tests: blood cell count,CRP,D-dimer( and transferrin,procalcitonin.).These blood tests should be obtained one time, before healthcare begin to have a contact,and then periodically,for to compare to first result of blood cells count.
I agree with Jon Blum. This is not such a simple question. Testing without tracing will ilkely offer many people a false sense of security. And without governmental economic support, those who can’t afford to miss work will likely keep positive results to themselves. I am not an epidemiologist but false negative rates over 15% don’t sound very reassuring to me.
Please what is the false negative rate for the so called gold standard PCR tests? Which brand of test is most reliable? How often does faulty collection technique or transport cause false negatives. This info in not clearly distributed to PCPs out in the communities.
Clifford Rosenberg, M.D. AAFP
The benefit of increased testing is finding positives. Negatives and false negatives would still be unidentified without testing. What is there to lose if individuals and/or high risk groups use a low yield positive test? I think many positive individuals would contact their physicians and self-isolate at a minimum. If a patient with a positive test is ill or in a high risk group, PCR can be done to confirm.
Test report should emphasize to the “negatives” that the test is not 100% and they are still susceptible and should follow the current public health guidelines.
The FDA approves much of dubious efficacy – see supplements!
If such a text were available schools or employers could require that student/worker take the test at home and show proof of negativity (via an app on their phones) before coming to school or work (or even for admittance to restaurants, bars, airplanes etc.)
If such a text were available schools or employers could require that student/worker take the test at home and show proof of negativity (via an app on their phones) before coming to school or work (or even for admittance to restaurants, bars, airplanes etc.)
The ability to have a rapid test is key to controlling the pandemic and has been known from the beginning. Unfortunately we do not have the leadership at a federal level that is needed to make this happen. It’s shameful and makes me furious. As a private citizen all I can do right now to protect myself, my loved ones, and people I come in contact with is to wear a mask, wash my hands, maintain social distance, and request my absentee ballot as soon as I can. I can only hope that a change in leadership will result in a change in priorities to combat the pandemic.
At-Home test kits are available now. They can test saliva or nasal secretions. Samples can be collected with video assistance if needed. Samples can be taken to a drop off site and immediate results obtained by point of care tests or overnighted for standard PCR testing. At-Home sample collection eliminates potential exposure from taking a symptomatic or at risk person for testing. It saves PPE now being used for sample collection. An impediment to the use of At-Home tests appears to be regulatory. My state (CT) has been running less than 1% positive tests for over a week, touting the low rate as a demonstration of successful control. But it is also a waste – we should be developing epidemiologic risk profiles, test smart, and using the resources being invested in negative tests and drive through sites for contact tracing.
Quite an interesting discussion here. Any test, antigen or antibody, is better than none. With any test, we can take it from there. The pandemic has raged on for far more than can be welcomed.
Dr.Sax is entirely correct. We must recognize that the present testing mechanisms, woefully inadequate to rapidly identify symptomatic patients, will never be able to screen a population of asymptomatic persons. A home point of care test with rapid results, is the only way to address this large cohort. Concerns regarding low sensitivity are spurious as few of these patients will undergo the traditional genetic tests, so it it is presumptuous to compare the two tests. While a negative test result may give some a false sense of security, an aggressive public service campaign educating society that a negative test doesn’t obviate the need for face coverings, social distancing and hand hygiene. A “true negative test” is only a snapshot in time and still requires the aforementioned prevention strategies.
Why not use this type of test and think outside of the box? How about a Fight COVID-19 week? This would be to identify every asymptomatic case and prevent further transmission.
1. Have the federal government supply everyone a box with 10 tests (and ability to request more if needed). At ~ 330 million Americans that would be 3.3 billion tests. At $1-$5 each that would be between 3 and 16 billion dollars (compare to the trillions spent on CARES and potentially more needed).
2. Pick a day when everyone will have the test kits. Everyone would do a test that day on themselves – I think most would do so especially if all of our “leaders” make it a patriotic action.
3. For those testing negative: a) they would re-test again in 3 days and 3 days after that (so 3 tests over 7 days). b) if they have symptoms then they would get a nasal/PCR test
4. For those testing positive: they would report and get a test number. They would isolate/quarantine themselves until they have 2 negative tests (? 2 days apart) … if symptoms, also until symptoms are gone. All they would need to do regarding contacts is contact people themselves and encourage/emphasize the contacts to test themselves. For those that will miss work – their employers will pay them as if they worked (8 hours/day) and the federal government will reimburse the employers with a simple form/application – mainly needing the person’s test number, number of days missed and salary.
Maybe the detection of Ags or Abs is not the adequate strategy. what about to think of and research of specific pulmonary mediators of the innate immune response using an in vitro assays? Maybe these ways will surpass the problem of false negative results for PCR.
I disagree. Why would anyone do a test at home that’s maybe ~50% reliable? Would any woman bother doing an at home pregnancy test if there is a 50-50 chance that it’s incorrect? No. The only thing better than bad data is no data at all.
Don’t ignore Bayes’ Theorem. This principle puts sensitivity and specificity in perspective. An asymptomatic repeatedly test-negative person would almost certainly be free of disease. A symptomatic test positive person likely has COVID-19. An asymptomatic person testing positive would benefit from more specific antigen testing to confirm infection. A symptomatic test-negative person would also benefit from followup testing.
The key is not sensitivity or specificity in this case, but post-test probability. The saliva test is quite appropriate for the screening use described.
Yes, exactly. We (or rather the FDA) did it wrong the first time. And they’re doing it again. I’m thinking the FDA doesn’t want people or companies putting forth anything unless it goes through the full-blown FDA approval/disapproval process, even if it takes years in the midst of this “emergency” pandemic, or even if that means that very useful things will never be put into use. They have the absolute authority and they mean to keep it, regardless of circumstances. It’s what they do. It’s who they are. Unfortunately for us. If I was developing this kind of test I think I would target another country. One that’s rich enough to afford the test, but not developed enough to have a bureaucratic not-invented-here attitude. It’s slightly possible that if the whole world uses such tests that the FDA might relent a bit. They didn’t do it initially for the WHO’s Covid-19 test, but it’s possible. Anything’s possible.
PCR tests are only about 70% sensitive. That’s bad enough. A test with an even lower sensitivity would just lead to increased false assumptions about who is and who isn’t infected. Backfire potential is huge. Could easily worsen the situation.
VERY MUCH INTERESTED, TO SAY THE LEAST!!!
“ Apparently, one thing that may be holding up FDA approval of these tests is that they are less sensitive than the PCR. That means they’re more likely than the PCR to miss someone who has COVID-19, wrongly giving a sense of reassurance from a false-negative result.” This is incorrect, FDA has set an 80% PPA/95% NPA vs PCR, which has been achieved by Quidel and BD so far — they will likely get better as well. The NPVs are quite good when looking at prevalence of 10% in the population. The WHO is also developing a Target Product Profile for PoC tests with similar performance for low & middle income countries. This point and the Mina article are dead right — we’ve got to get past this PCR obsession; it is using a sledgehammer when a scalpel will be sufficient.
What sensitivity and specificity do you consider? 90% and you miss 10%. 80% and you miss 20%. Contact tracing has got to be done. Masks are essential. Staying out of crowds and distancing are essential. The problem is that to many want immediate gratification in the form of medical clearance. To many think it can’t happen to them. And being negative today after an exposure does not mean you will be negative tomorrow.
If your privacy is putting others at risk, you loose your privacy. Same things goes that your civil rights end where mine begin.
Ernest M Kraus, graduate pharmacist
This is already being worked on as an open platform approach in the Gates Foundation.
What would be an acceptable rate of false negatives?
The antigen test are abysmal, false negative rates of almost half in some
I fail to understand why anyone would want to push for a test that they know; has a low sensitivity.
What’s the point if a lot of people with negative tests are actually false negatives and will be out there infecting others unknowingly with this false sense of assurance with such a test.
We must develop a strategy that overcomes the current paralysis afffecting our society
Formal PCR testing for those who are symptomatic and close contacts of confirmed cases should continue
Home saliva antigen testing, perhaps blue tooth enabled, would allow more widespread testing and reduce demand on pathology services
We have to develop a rapid health indicator that stops the lockdown of an entire community when very few are affected
As Dr Sax suggests have a test an hour before you go to an event or board a flight
We have to be smarter than isolating all as if we are facing the plague
I agree that the sensitivity of rapid home tests are sufficient for broad testing of specific populations. However, I would propose taking “home” out of the equation.
Is there any reason why rapid molecular tests can’t be deployed using the drive up testing site
set-ups?? This way the results are recorded and reported to the health department with case information so contact tracing can be initiated. The lines and waits would not be as long, the use of PPE’s may be reduced and the results returned more quickly…etc.
I have to say I’m not a fan of depending on the bluetooth connection to Covid19 home test results. I say this as a retired Supervising Communicable Disease Investigator, HHSA, Public Health Division of Infectious Diseases for 25 years. A confirmed diagnosis can be a scary experience for many people. Immediate contact with trained public health personnel provides support and education as to the next steps in taking care of themselves and protecting others….including initiation of contact tracing. Many people are much more likely to give contact information when they know they will not be named as the index case. Trained personnel know how to zero in on the time frame when the index case was most infectious and get contact information. Many public health(PH) divisions have support staff to provide the necessities so the index case can isolate with less worry about how basic needs will be met. My experience with individuals who needed to isolate (primarily infectious TB) don’t always stay isolated. PH involvement has the weight of legal orders of the local Health Officer when an individual continually ignores a specific directive. It is often the last resort to restrict a persons’ free movement and it is not taken lightly by PH staff. These are opportunities lost when the case is not reported to the local health department.
Public health staff is well aware of this aspect of human nature. They recognize that all of us take calculated risks..like Rand Paul, a US Senator..who suspected he had Covid19, went for a test, circulated in the capital for 6 days and only isolated when he received his positive test results. But PH involvement brings experience, resources and some pressure with the thumbs to quicken the suppression of the virus. This is of course the opinion of a PH staff member who was in ground zero for SARS in 2003…..I believe the connection is vital as well as these rapid tests.
I am also aware that the CDC case definition of Covid19 included confirmed as well as presumptive cases. It is beyond me why presumptive cases were not followed up by local health departments as well as confirmed cases, especially in the beginning when molecular tests were in such short supply. I do understand that this pandemic occurred alongside the influenza season. But the advantage of treating presumptive cases like confirmed cases would be to reduce the continual transmission of Covid19 as well as influenza. Less case transmission early on could have lessened the burden of disease to a community.
I also agree the frequency of testing is key…especially since the technology and staff needs are reduced with the rapid home tests, as well as the costs. These tests can be put into play in congregate housing situations where physical distancing is not easy to arrange such as prisons, meat and poultry factories. As soon, as you can test remove and isolate a person with a positive test result…the more likely a community can suppress the virus enough to slowly and cautiously resume re-opening. Rapid tests of circulating viral levels could provide decision makers reliable, if not perfect measures for adjusting the re-opening phases. So not being able to catch all the fish at one point does not preclude catching most of the fish most of the time in order to know where we stand.
There is no doubt in my mind that more testing will pick up those elusive asymptomatic persons. We already know that these individuals are being picked up as testing occurs prior to any invasive medical or dental procedure requiring close contact. We picked up out first pediatric case this way and the infectious parent who was an EMT. So one can see with a variety of testing modalities…the symptomatic and asymptomatic cases can be captured. This is the goal…rapid capture of infected individuals, public health intervention with contact tracing strategies ….all efforts reduce the amount of circulating virus In a community.
I was under the impression that the above tests are approved as Emergency Use Authorization (EUA) by the FDA….so when you are talking about FDA approval are you speaking about a more throughly vetted process than EUA??? In fact, aren’t all the current molecular, antigen and antibody tests all authorized under EUA at this point in time??
The dilemma with these tests is this:
The positive ones can isolate even if they are falsely positive.
The negative ones will have to retest and retest until they become either positive or they become tired and frustrated.
In the end, the best test may be to assume everyone, including yourself, is positive. And utilize the Covid-19 “condoms”
It will be much more helpful for developing and highly dense population countries.
The very many well focused comments I’ve just read underline 2 enormous currents: A) humans desperately trying to look for answers to precise early diagnosis, adequate therapy and prevention of COVID19 infections. B) humans incapable to fathom the depth of the problem and, due to numerous reasons, keep contaminating or infecting fellow humans. All these is happening world wide.
This unique pandemic has revealed how unprepared to face it are Health Care, Economic and Political systems and at present nobody can anticipate the way of life is waiting ahead of us. Taking into consideration what I said at the beginning I guess Darwinian laws could prevail for the foreseeable future. There is however a final concept I would like to share with you and it is this: the entire universe is regulated by a dynamic, ever balancing “critical mass”. a few examples starting with the human: Pregnancy time 9 months more or less than 9 months means danger, giving a vaccine: if it has too much antigen can be lethal, if it has little antigen it does not work. and if we go at deeper molecular levels of analysis the whole thing becomes pure mathematics. Cities, Le Corbusier a Swiss architect suggested that the cities of the future should not have more than 200,000 inhabitants, the buildings should be built on pillars so there should be grass and gardens on the ground at the “cows should grassed peacefully down below” in other words Le Corbusier was suggesting to maintain the critical mass for cities and balance the interaction between humans and nature. Look at the cities today! smaller cities would have made this pandemic more manageable. One can go one for ever with more examples, Finally, unlike before the pandemic, now we no nothing about what the future has in store for us however, I believe that is we, as humans want to survive, we have to redesign our entire existence on the basis of determining what “dynamic critical mass applies” for everything we do from now on. It will take a long time and effort but it may relieve the chaos and pave the way for a more sustainable existence with Nature on our side.
I think the game changer is a rapid test at the door. The door of a plane or restaurant or job or bar or hospital. What if you knew everyone in a “space” was negative, then no need for masks or social distancing. A 5 – 10 min turnaround time test gets us to this place. Of course would have to be inexpensive and available in billions of units. Am I dreaming? I did read a few weeks ago of an Israeli inventor working on a test like this where the person blows in a tube and haven’t heard more about it.
Recently testing has been up-scaled substantially in Delhi, India – mainly with introduction of antigen kit (SD Biosensor) with low sensitivity and high specificity.
Apart from parallel up scaling of isolation beds – largely other conditions remained the same.
Delhi is experiencing sustained decline in daily incidence since this up scaled testing strategy.
Rapid home tests are exactly what we need. Our current handling of this virus makes zero sense. Taking a test at home any time you are going out in public and receiving results within an hour does. The FDA needs to get this approved NOW!
I couldn’t agree more. The only way to contain the transmission is to test EVERYONE without symptoms. A cheap, readily available home testing kit can achieve this. I agree that antibody tests are not the answer. But we now have RAPID ANTIGEN TESTS that results in 15 minutes. Sensitivity may be slightly lower than the PCR but still not bad. The lower sensitivity can be overcome by increasing the frequency of testing. Three consecutive negative tests will increase sensitivity and minimize the false negative rate significantly. But it will allow asymptomatic people to know if they are infectious before they go out to see an elderly relative or attend other important business without the risk of transmitting the virus to other people. Until will find an effective antiviral with near 100% cure rate this will facilitate opening up the economy without risking infection rate. I am a physician and a patient who recently tested positive for SARS-COV2 virus and in self-quarantine.
Can Dr. Sax or The NEJM give us a list of all available tests and their specificity and sensitivity ranges?
If there are significant variations within each test ,
as well as between different test,
and many different tests are being used,
by different testers,
how can we make sense of the results???
Also people without cars, computers or the resources that many of us take for granted will not be able to avail themselves of drive through testing sites. They might not be able to afford home testing at $5.00 a pop, let alone repeating false negatives X3.
And these are the people who are most vulnerable to death from COVID.
We need good clear info. We need Public Health Involvement. We need Contact Tracing and Isolation. We need mobile testing to reach out to the poor.
We need to sacrifice some privacy and convenience, like our parents did during WWII.
What good is an open economy if a significant part of the consumers are dead or disabled by COVID? Let’s see if the states that have driven down case numbers with lock downs can maintain that with other state exploding.
Until we get definitive treatments or vaccines, we will need to be safe, vigilant and compassionate.
Thank you everyone for your passionate discussion and involved. I just want to point everyone’s attention back to Sam Slonim’s strategy of picking a “COVID-19 “I have taken the liberty of copying his plan below:
Sam Slonim
July 11, 2020
Why not use this type of test and think outside of the box? How about a Fight COVID-19 week? This would be to identify every asymptomatic case and prevent further transmission.
1. Have the federal government supply everyone a box with 10 tests (and ability to request more if needed). At ~ 330 million Americans that would be 3.3 billion tests. At $1-$5 each that would be between 3 and 16 billion dollars (compare to the trillions spent on CARES and potentially more needed).
2. Pick a day when everyone will have the test kits. Everyone would do a test that day on themselves – I think most would do so especially if all of our “leaders” make it a patriotic action.
3. For those testing negative: a) they would re-test again in 3 days and 3 days after that (so 3 tests over 7 days). b) if they have symptoms then they would get a nasal/PCR test
4. For those testing positive: they would report and get a test number. They would isolate/quarantine themselves until they have 2 negative tests (? 2 days apart) … if symptoms, also until symptoms are gone. All they would need to do regarding contacts is contact people themselves and encourage/emphasize the contacts to test themselves. For those that will miss work – their employers will pay them as if they worked (8 hours/day) and the federal government will reimburse the employers with a simple form/application – mainly needing the person’s test number, number of days missed and salary.
Sona Nanotech, one of the companies listed above, has developed a home antigen test with 96% specificity and sensitivity. The test takes 15 minutes for results. They have partnered with a company named Bond which has an app based platform which provides health authorities with a real time data. They have pre-sold several million test kits pending regulatory approval. The test would do everything everyone wants if it’s approved. It is expected to cost $50 per kit. That is inexpensive compared to PCR testing which takes 24 hours at best (meaning if labs have the capacity to process them). It should provide a safe path for businesses to reopen and safety for employees who are presently working. Sona claims it could receive clearance from some regulators by the end of this month. Here are some links.
https://sonanano.com/sona-nanotech-announces-validation-results-for-its-covid-19-antigen-test/
https://sonanano.com/partners/
https://sonanano.com/covid-19/
This is an excerpt from the first link: laboratory validation studies of performance levels have resulted in a test sensitivity of 96%, test specificity of 96% and a Limit of Detection (“LOD”) of 2.1 x 102 TCID50. Sales of the tests will now be permitted under a ‘research use only’ label until full regulatory authority is granted, in relevant territories, at which time the ‘research use only’ label requirement would be lifted, as discussed below. Technology transfer to manufacturers is currently underway to produce tests to meet current and expected demand. The Company will provide an update on sales progress and manufacturing delivery timetables in the coming weeks.
MRIGlobal, using live COVID-19 viral cultures, determined the test to have a limit of detection of 2.1 x 102 TCID50 which corresponds to an ability to detect the virus in patients with ‘low’ viral loads in 10-15 minutes, as compared to RT-PCR testing which typically takes 24-48 hours to detect the virus. Limit of detection is the minimum amount of target microorganisms that can be reliably detected under optimal conditions and is an essential step in determining the sensitivity of any assay. Current studies show positive COVID-19 patients presenting symptoms have viral loads in the 104 – 106 range.
Validation studies were also conducted in-house to assess potential clinical performance of the test using 30 nasopharyngeal samples from healthy individuals who were presumed negative for COVID-19. Results from the study generated a specificity of 96% (29/30) and a sensitivity of 96% (28/29). All specimen samples tested generated negative results, except for one, generating the above result of 96%. To generate the sensitivity data, the remnants of each negative sample were spiked with gamma irradiated COVID-19 virus and the tests rerun to determine the positive results, generating the above result of 96%.
As the pandemic continues and the understanding of COVID-19 improves, regulators have placed greater emphasis on clinical, ‘in-field’ evaluations of rapid tests at the point of care to ensure they can be deployed with confidence. Following consultation with MRIGlobal and the FDA, Sona will enter into independent clinical, in-field evaluation studies to generate the data to support its analytical and clinical data as part of the submission it will make to Health Canada and the FDA for emergency use authorization (“EUA”) approval. In-field collection of a minimum of 30 confirmed negative and 30 confirmed positive specimens and the associated data analysis is expected to be completed while technology transfer to manufacturers is still underway. To that end, the Company has engaged with a contract research organization (“CRO”) based in the U.S. to conduct one such study and a university-affiliated laboratory outside of the U.S. to conduct a second. The Company has been informed that the results of these field studies should be provided by the end of July, at which time it intends to make final submissions to regulatory authorities in multiple jurisdictions. During this time, technology transfer will continue and quality assurance manufacturing batches are expected to be run with manufacturing partners. The Company is committed to maintaining ongoing evaluations of its test in order to understand its performance in a wide range of testing environments.
I have a Garmin watch, Venu, measures oxygen%….
Has anyone done any studies on the level of oxygenation in non-symptomatic covid cases….
And, whatever happened to social distancing… without testing, just all of us behaving ourselves and staying distant. Except for frontline, and then no facial hair n-95 or better…
I think that the world should just be more patient, and the testing shows you are ok, just for that day, so everyone has to keep testing every day, 7 billion tests each day? What are you talking about?
This is in continuation to my response above dated 12 July 2020.
The antigen test reported is – rapid point of care kit for covid 19 antigen (Standard Q). Gives result in 30 minutes.
Since substantial up scaling of testing with use of this kit in Delhi, India, there has been a sustained decrease in number of new cases reported daily – with decrease in active cases.