
An ongoing dialogue on HIV/AIDS, infectious diseases,
October 4th, 2020
Does the White House Outbreak Invalidate the Strategy of Frequent Testing for COVID-19 Control?
As I’ve written here many times, I’m hopeful that frequent, inexpensive, rapid home testing for COVID-19 will help us climb out of this pandemic mess.
Let’s name it the Mina Frequent Testing Plan, after my indefatigable colleague Dr. Michael Mina who has championed it for months — most recently in a perspective published in the New England Journal of Medicine.
For the Rip Van Winkles out there, here are the basics of this approach:
- Much of the community transmission of SARS-CoV-2 comes from people who don’t know they are infectious since they have no or few symptoms.
- Testing them using standard PCR tests is impractical — too slow, expensive, and difficult to access.
- Scientists and companies have collaborated to develop simple paper-based rapid tests done on saliva samples.
- Results return in 15-30 minutes and require no special instruments for interpretation — analogous to home pregnancy or HIV tests.
- Produced at scale, the tests are cheap and readily available — $1-5 each.
- These tests pick up some people who have high levels of infectious virus but are either asymptomatic or presymptomatic — hence potentially contagious to others but otherwise unaware themselves. Now, none of these people are being detected.
- Once they have a positive test, they isolate at home — they don’t go to work or school. Tests would be confirmed using standard PCR.
- Individuals can also buy them for use at home.
- Schools, hospitals, nursing homes, food service companies, places of worship, and others can purchase them in bulk, with requirements for a negative test (even better, a series of negative tests over the previous several days) for entry.
The strategy has a growing number of advocates across the medical, scientific, and public health fields — including the FDA — which is exciting. Here’s a short white paper on the topic many of us have helped draft, with a focus on testing in schools.
But as the Mina Frequent Testing Plan drew sufficient attention, various criticisms appeared, in the press and on social media. (Here’s a skillful rebuttal.)
These negative views certainly raise important concerns. I worry in particular about false positives — they will be inevitable when doing high-volume testing on a low-prevalence population.
Now, we have a president who acquired COVID-19 despite the fact that he and those who surround him are tested often.
How did this happen? Is this the death knell of the Mina Frequent Testing Plan?
The obvious first explanation is that no test is perfect. The rapid antigen tests used by the White House will miss some people who are infectious. Of particular concern are those who get tested only once, right before meeting the president.
The math is simple — if you increase the number of visitors, you increase the chance that at least one person with infection will escape detection with a single rapid test.
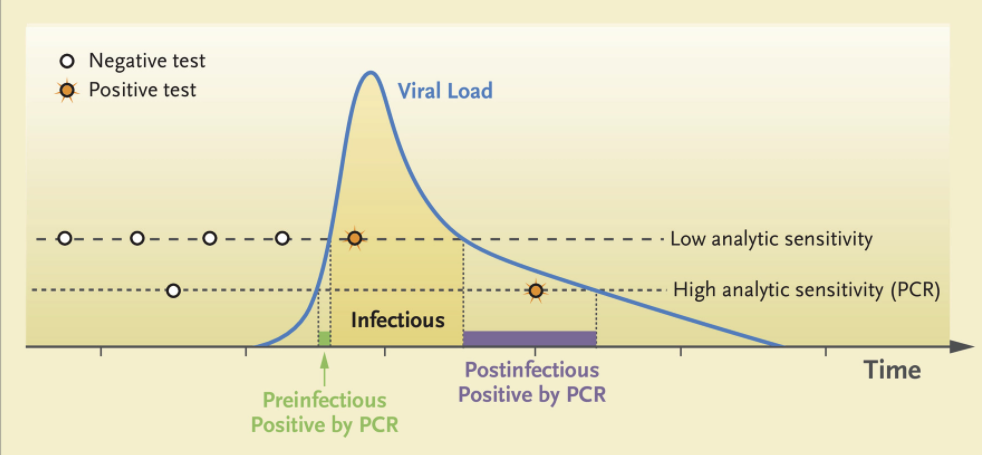
Remember, one strength of the Mina Frequent Testing Plan is just that — it’s frequent! People who test negative in the early phase of infection will test positive with tomorrow’s or the next day’s test based on the kinetics of viral replication in someone who has just come down with the disease.
From Mina’s NEJM piece, here are those viral trajectories — a person with a negative test in the morning could potentially be infectious shortly thereafter:
With the many visitors to the White House on Saturday, September 26 — the day the president announced the nomination of Judge Amy Coney Barrett to the Supreme Court — only a single rapid test granted them access to the event, mask-free.
Also, let’s remember that testing won’t give us a free pass to behave as if we were living in the Before Times, again because testing isn’t perfect. Certain activities facilitate spread of the virus — crowds, close conversations, poor ventilation.
How about this for an example?
At least 7 people who attended ACB's nomination ceremony in the Rose Garden on Sep. 26 have since tested positive for coronavirus. But experts say the more risky time spent that day was at a reception inside the White House. Here are some scenes. https://t.co/mTsZsxmSfy
— Christiaan Triebert (@trbrtc) October 3, 2020
Ouch.
Or this?
Double ouch! Watching that video makes most of us ID clinicians feel like we’re living on another planet. Suspect many of you readers feel the same!
In summary, let me quote my Boston ID colleague Dr. Roby Bhattacharyya, who wisely wrote:
People tap-dancing prematurely on the grave of rapid testing should reflect on how remarkable it is that for people behaving this way all year, indoors and out, in a place with countless thousands of visitors, it took until October for a superspreading event to happen. Test more.
So yes, the Mina Frequent Testing plan lives on — even if the track record of keeping the president free of the virus does not.
Which teaches us more about the limits and vagaries of human behavior than it does the limits of testing, doesn’t it?
20 Responses to “Does the White House Outbreak Invalidate the Strategy of Frequent Testing for COVID-19 Control?”

Paul E. Sax, MD
Contributing Editor
NEJM Journal Watch
Infectious Diseases
Biography | Disclosures | Summaries
Learn more about HIV and ID Observations.
 NEJM Journal Watch — Recent Infectious Disease Articles
NEJM Journal Watch — Recent Infectious Disease Articles- Observations from ID and Beyond: Federal HIV Guidelines Face a Shutdown — A Critical Loss for Clinicians and Patients
- Ceftriaxone for Patients Hospitalized with Pneumonia: One Gram or Two?
- More PrEP, Less HIV: U.S. State Data
- Observations from ID and Beyond: Why the Sudden Firing of ACIP Members Should Put Every Clinician on High Alert
- Does HIV RNA Testing to Monitor PrEP Add Value?
Wow, I’ve finally made it as an ID doc to have a Tweet in JWatch! Isn’t that how this works? Anyway, my 4-year-old daughter saw that video over my shoulder as I was writing that tweet, and she said, “Is that for real? They shouldn’t be doing all that hugging!” So… yeah.
I am a Mina disciple so thanks for this. I believe the president has too many exposures to unique individuals. A defined cohort should have been used and they should be tested daily. I also suspect they may have drifted away from testing the POTUS and relied on single tests of those coming in contact with him. From where I sit the POTUS may be the super spreader. If so – he wasn’t getting tested on a set schedule with enough frequency
Paul,
As I have posted here before, that way lies madness, and keeps us beholden to this CCP virus for the indefinite future. Maybe that is what you all academic phyisicians want at least until November 3, 2020.
The best way to get past this virus is for as close to everybody in the country, if not the world to become immune to it. Natural infection is the way to do tha: strong long lasting immunity (both humeral and cellular such that measureing humoral immunity underestimates true immunity. Every virus (except HIV) known to man–here I may exaggerate, but it is true for Corona viruses) provokes a strong long lasting immunity to the strain/serotype that one gets infected with. (e.g., once infected with Type 1 polio, a person doesn’t get it again (Type 2 & type 3 being a different story). Immunization generally does not provoke as strong and as long lasting an immunity (hence minimum 2 doses for each vaccine in the required childhood vaccines (and Hepatitis A vaccine). (Yellow Fever is the only exception that I know of.)
The only vaccines that are accomlish anything like herd immunity are those that are enforce on pre-school and school children (rational public health reasons and laws, but probably only enacted because children can’t vote, and can’t effectively vote with their feet to refuse). Even then their antivaccer parents have carved out exceptoins beyond the 1st Amendment necessities to frustrate attempts at compliance.
With the flu vaccine as a model ( uptake generously self reported to be 33–56%, average of 45% & we all know how reliable self report is , especially when being queried by some one asking about a health question by a health agency, & the only figure that I could find is the number of doses distributed (~170 million in US ~50% of US population) but that is distributed, not administered.
Doing the math: 0.5 (vaccine effectivness required to be licensed) x .45 avg uptake of flu vaccine as proxy = .225 (22.5%) population immune–(and for how long?); being optimistic (.66 vaccine effectiveness) .66 x .45 = .297 (29.7%) of population immune. And there will be a spread of compliance in different communities: my personal experience talking with patients is that there is at least a 20-25% intend not to take the vaccine (small biased sample).
It is time to organize COVID parties, just like we as parents organized Chicken Pox parties for our kids (I wil be 70 in 2 months). We could start on college campuses. No need to organize the students will do it themselves.( they certainly are not going to social distance on their own accord–STDs on college campuses ring a bell?) By Thanksgivng time the whole cohort will be immune to COVID-19 and they can celebrate Thanksgiving with Grandma and Grandpa (great grands as well) in complete safety for the elders. Instead spineless adminstrators are sending kids home and shutting down campuses. Why do the administrators hate their student’s grand parents so much?
Protect the elderly and elderly sick as much as they will let you and give us our freedom back, and don’t spend money that the government does not have on a fool’s errand.
You all have your hands full with HIV and with antibiotic resistance.
Have a nice day.
Dear Dr. Kimber,
I agree the solution is herd immunity, but we should do it through vaccination. Trying to quickly infect 300+ million people would result in huge numbers of hospitalizations, overwhelm hospitals with an associated spike in the mortality rate, and millions of dead Americans. There is also a good chance it wouldn’t work: your premise that coronaviruses must induce long lasting immunity is false (for example, see Eldridge et al, Nature Medicine 9/2020; reinfections with seasonal coronavirus were common by 12 months). We should try to keep a lid on this virus as much as possible, while intelligently opening as much as we can safely. But COVID parties? No sir.
How many positives were there of all those tested for the Sept 26th White House event? None? And obviously we can see the “large number” of possible false negatives in the pictures. But we assume they were true negatives on that Saturday. Are there any “controls” to insure the test is correct?
Since there is so much high quality video, it would be easy to quantify everybody’s known contact with everybody else. This is a golden opportunity for some high quality research using a “natural experiment” of behavior that would never had been permissible if somebody proposed a study of transmission among people who tested negative but flouted rules of social distancing. I hope somebody is studying it.
and sequence the virus of all these people
“Once they have a positive test, they isolate at home — they don’t go to work or school.” That is the problem, Trump was symptomatic and clearly had a known positive Covid test before he announced it on Friday (Saturday morning his physician said he was “72 hours into the illness”- oops!), but he still went about his daily activities, interacting with people without a mask and putting them at risk. Recall that the Trump entourage arrived at the Tuesday debate TOO LATE to get the rapid test. Presumably that is because they knew some of them were positive for Covid but did not care about infecting others.
Rapid testing is a great idea, but we need everyone – including our leadership – to agree to participate in the system.
Unfortunately while a good idea–frequent testing–in and of itself is insufficient for epidemic control. The Abbott ID Now is just not a great test for detecting early infection. Why the White House did not go with a 8-12 hour PCR testing program is a mystery and perhaps another foolish mistake by folks who do not know what they are doing.
Rapid Antigen tests detect moderate and high viral load cases and is an excellent tool in a high prevalence population. It misses out asymptomatic and pre symptomatic or mild symptomatic cases. Important to understand that these cases do transmit the disease, specially in a congregation.
Dear Dr Sax I am amazed at the credulity of people who question the efficacy of testing in asymptomatic people.The only way out of the mess we are in is by universal tests done on
Everyone..The availability of inexpensive antigen based paper tests using saliva makes this
A reality..I feel that identification,isolation and internment of asymptomatic carriers will prevent
The super spreaders.and the virus rill an effective ,safe and in expensive vaccine is available.
With regards
Dr Ramesh
the need for a rapid and cheap test for SARS-CoV2 is evident. While accuracy for both false positives and false negatives is important, it is less so given the inability of current nasal swab tests to cover even a fraction of the need for increased testing. It may be that the Mina approach will not work on an individual basis, but is more important for identifying potential clusters before they develop. If I were going in for a test I would elect the somewhat uncomfortable nasal/throat swab, but if I were administering the opening of a school, quick and frequent testing could be the tool to accomplish it.
My issue is with the following statement “Schools, hospitals, nursing homes, food service companies, places of worship, and others can purchase them in bulk, with requirements for a negative test (even better, a series of negative tests over the previous several days) for entry.”
I have now been testing positive for three months after having the virus in June. I am trying to have a surgery.
I think frequent testing of asymptomatic persons for COVID-19 is useful, but as I and even my non-physician family members have realized, one can test negative one day and positive the next. Frequent testing is only one component of an overall approach to preventing the spread of COVID-19. Wearing masks and social distancing are absolutely necessary. Unfortunately, many people still rebel at this idea.
Oh Paul. Call me a cynic. But the key to rapid testing control is not the testing, it is the follow through. And my experience with human nature doesn’t allow me to believe for a second that human primates are selfless enough to adhere to the stringent protocols required for control. There are always important things to do, people to see, paychecks to earn, voters to snow, etc. etc. so many little exceptions that justify a big breach, in all arenas of human activity. Didn’t HIV tell us that once already?
sadly, az
Right on as always, Paul Sax: ” I worry in particular about false positives — they will be inevitable when doing high-volume testing on a low-prevalence population”.
From what I have read, the White House has been using the ID NOW isothermal nucleic acid detection test, which, supposedly, is in between antigen detection and “traditional” PCR in terms of lower limit of detection, at least when NP swabs are used. I wonder about the quality of specimen collection.
I also wonder whether some of the President’s contacts have not been tested, for whatever reason.
Frequent testing is ok. But the idea that a positive test will AUTOMATICALLY CHANGE BEHAVIOR is false. Many people have gotten a positive result and continue to go about their business because they don’t care. Their day is more important than some else’s life.
Isn’t this all being made more complicated than it needs to be? How about a major public health campaign whereby society makes it unacceptable to be out when one has any mild “viral” symptoms – be it a sore throat, hoarse voice, new runny/congested nose/sneezing, not just a cough or high temperature. Yes some of these folks won’t have COVID but much simpler than trying to interpret meaning of tests. Do we know what is the proportion of cases spread from those with mild symptoms, as opposed to really being asymptomatic? (My hunch is that most COVID infection transmission is from those with mild symptoms).
75% of the workforce would be in quarantine at any given time if we abided by this option. Seems illogical. Half the time I hear someone has a sore throat, my throat immediately becomes sore and I am not one to panic or exaggerate as many that I know are. If we want to completely shut down again for 30 days, we will just be shut down for 30 days and the virus is still there. Protect our most vulnerable and for those with little to no symptoms-no harm done. Wear a mask when in close contact. POTUS needs to emphasize this and not demonize it.