
An ongoing dialogue on HIV/AIDS, infectious diseases,
September 8th, 2022
A Back To Work ID Link-o-Rama

Zelda, Zoe, and Louie on the cover of their latest album, Parallel Paws. With apologies to Debbie Harry and Chris Stein.
A few nuggets are rattling around in the inbox post Labor Day, including this extraordinary photo of our family dogs Zelda, Zoe, and Louie, posing for their latest album cover.
Woof!
Besides, I haven’t done one of these Link-o-Ramas since January 11, 2021! That was either 20 months ago or 20 years, hard to keep track of time these days.
Enough with the introduction. On with the links — starting with some highlights from this year’s 2022 AIDS Conference in Montreal:
- Should people on PrEP or with HIV with a recent history of bacterial STIs take doxycycline post-exposure prophylaxis after sex? The cleverly named doxyPEP study showed a marked reduction in all bacterial STIs, including gonorrhea — a benefit not observed in a similar study conducted in France. And living in New England, I am, of course, reminded of post-tick bite doxycycline every time I hear about this strategy!
- Treatment of people with HIV/hepatitis B co-infection with BIC/FTC/TAF led to more favorable hepatitis B outcomes at 48 weeks than TDF/FTC plus DTG. These results suggest that TAF should be preferred over TDF for coinfection treatment. FYI, these were two of the three potentially practice-changing studies presented at this year’s 2022 AIDS Conference. (The third study, using injectable cabotegravir-rilpivirine in PWH with viremia, I’ve covered in more detail previously.)
- Another person with HIV has been cured with a stem cell transplant from a CCR5-negative donor. While this “City of Hope” patient with AML is just the fourth (or fifth, if you count the mystery Dusseldorf patient) to be cured, each cure case adds to our understanding of how we might accomplish this one day with more practical methods.
- This example of “exceptional” HIV control may give us an alternative to a sterilizing cure of HIV. Diagnosed with acute HIV in the 2000s, with a baseline HIV RNA of 70,000 and CD4 of 800, she was treated with ART and a grab-bag of immune based therapies (cyclosporine, IL-2, interferon, GM-CSF). Now off ART for more than 15 years with stable CD4s and an undetectable HIV RNA, she has a steady decline in the HIV reservoir with “enrichment of memory-like NK cells and CD8+ gamma delta T cells with NKG2C.” Sure. As always with such isolated cases, how much can we attribute to our interventions, and how much to a one-off very fortunate immune response?
- Targeted versus “shotgun” metagenomic sequencing on sonicate fluids derived from patients with suspected prosthetic joint infection had comparable yields, with the former being less expensive and having a faster turnaround time. Note that it detected potential pathogens in 48% of culture-negative PJIs. How long before such molecular testing becomes standard of care?
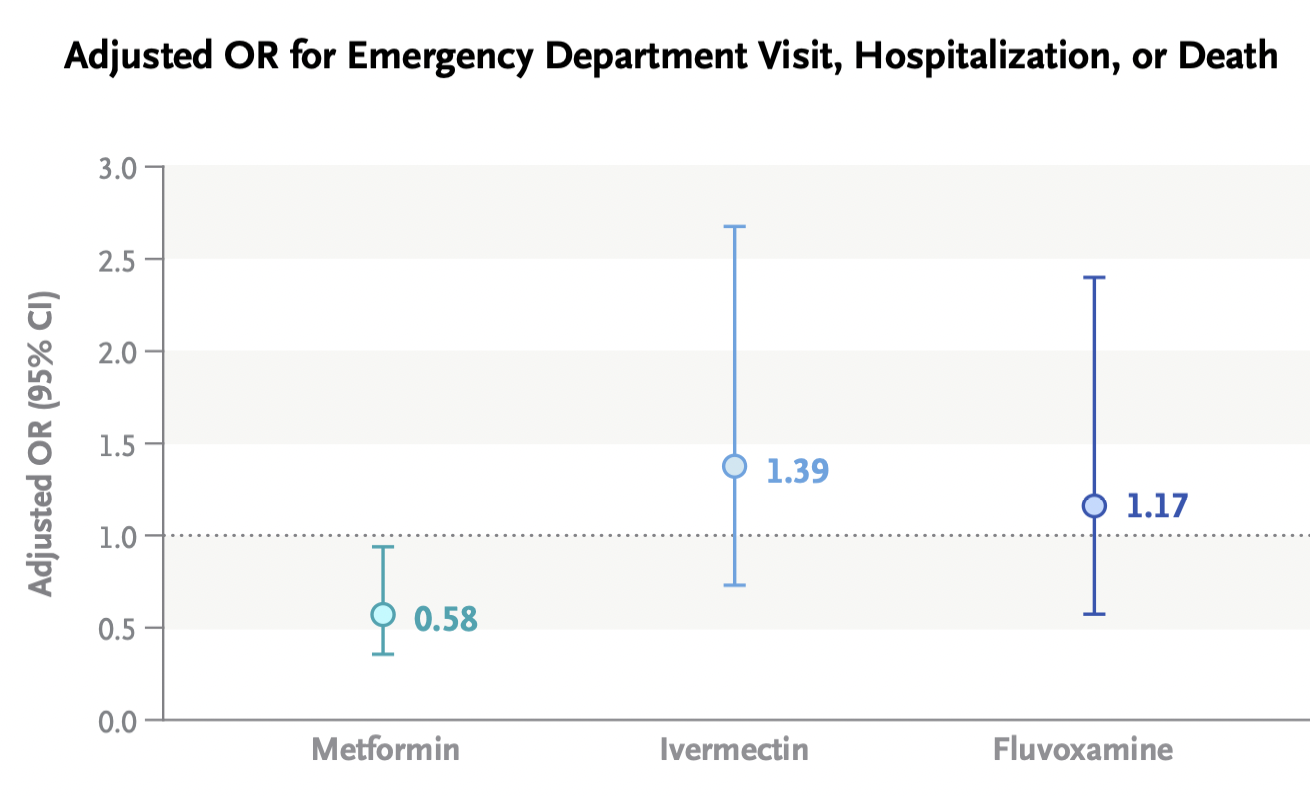
- A randomized clinical trial comparing ivermectin, fluvoxamine, and metformin to placebo for outpatients with COVID-19 found no significant difference in the primary outcome compared to placebo. One can be encouraged, however, by this signal from the metformin arm by looking at the secondary outcome of emergency department visit, hospitalization, or death. For a detailed further discussion of this interesting study by Dr. David Boulware, a co-investigator, read here. Note that a higher dose fluvoxamine strategy (which worked in the TOGETHER trial) is part of the ongoing ACTIV-6 clinical trial.
- Metformin shows up in numerous ID-related studies. In addition to its pleiotropic endocrine and anti-inflammatory effects, we can add antiviral activity against KSHV, SARS-CoV-2, Zika, and dengue, and a potential adjunctive role in tuberculosis, among others. And if you want to go further down this metformin rabbit hole, it’s not just being looked at for infection!
- A systematic review suggests that doxycycline for community-acquired pneumonia could make its way into the next guidelines. Resistance to azithromycin and the toxicity of fluoroquinolones make this a highly desirable option. Great accompanying editorial by the legendary Dr. Daniel Musher.
- Do either vaccination or prior infection reduce a person’s infectiousness when they contract COVID-19? Once we get past the fact that neither eliminates the risk of transmission — nothing is 100%! — we can at least cite several studies that prior immunity to SARS-CoV-2 reduces transmission risk, including this recent one done in a prison setting. Such data may point to a more stable time without marked surges, as community-wide immunity from either vaccine or infection or both could flatten rapid spikes in transmission.
- China has approved an inhaled vaccine for COVID-19. Used as a booster strategy after prior vaccination, the adenovirus-based vaccine induced humoral, cellular, and mucosal immunity. It’s the mucosal immunity that we hope will be more effective in blocking infection than our current vaccines. This is a big challenge, so it’s fortunate that many — around 100! — inhaled vaccines are under investigation.
- Are we treating peripartum infections appropriately? This review appropriately challenges the 2017 American College of Obstetricians and Gynecologists (ACOG) guidelines, which remarkably (and weirdly) still recommend ampicillin (or clindamycin) plus gentamicin — despite the fact that resistance to ampicillin is common, the dosing of these two drugs is complex, aminoglycosides penetrate poorly into abscesses, and the longtime availability of several safer and likely more effective options — such as piperacillin-tazobactam. “Get with the times” indeed!
- Treatment of cerebral toxoplasmosis with TMP/SMX appears to be as effective and less toxic than pyrimethamine and sulfadiazine. It’s also way less expensive, and much easier to take. This excellent systematic review could (some would say “should”) be guidelines-changing, as there is unlikely to be another prospective clinical trial conducted anytime soon, and most of the world already has made the switch.
- People who inject drugs admitted with complicated S. aureus bloodstream infections (including endocarditis) should be offered oral antibiotics at the time of discharge if they can’t safely continue intravenous therapy. Outcomes are significantly better than no antibiotics and comparable to IV after 10 days of IV treatment. Some would say switching to oral therapy should be the default option already — for everyone, if possible.
- In pregnant women, dolutegravir-based ART was superior to atazanavir–ritonavir, raltegravir, or elvitegravir–cobicistat in achieving viral suppression at delivery. It was similar to darunavir- and rilpivirine-based regimens, but the former is suboptimal due to twice-daily dosing, the latter because of food requirements and contraindicated acid-reducing therapies. With dolutegravir as the preferred option right now, we urgently need similar observational data on bictegravir/FTC/TAF, which is extensively used in clinical practice.
- Should linezolid replace clindamycin as adjunctive therapy for severe group A strep necrotizing fasciitis and toxic strep syndrome? Rates of resistance to clindamycin among beta strep species are high, and linezolid has similar in vitro suppression of toxin production. Makes sense. But file this one under the long list of questions for which there will never be a randomized clinical trial.
- SARS-CoV-2 spike antigen was detected in a majority of patients with long-COVID, or PASC. In 12 who had longitudinal samples, detection lasted 2-12 months. These results, if confirmed, imply a persistent reservoir of active viral replication, viral antigens, or both — and could lead to diagnostic tests and treatments, both of which are now sorely lacking.
- A clinical trial in the United Kingdom is testing tecovirimat treatment for monkeypox infection. Conducted remotely, with any clinician eligible to refer participants, the PLATINUM study tests tecovirimat 600mg twice daily for 14 days versus placebo on the rate of recovery and time to viral clearance assessed by weekly self-taken swabs. A similar study in the USA, run by the ACTG and called STOP, is expected to start soon.
Non-ID section:
- Even non-tennis fans might like this 2012 story about Frances Tiafoe. Written when he was just 14, the piece describes the childhood of the now 24-year-old Tiafoe, the first American man to make US Open semifinals since 2006. Stories like this definitely make me feel more patriotic than any shallow flag-waving! Tiafoe will certainly have his hands full tomorrow when he faces tennis wunderkind Carlos Alcaraz!
- A cardiac surgeon continued to operate despite a record number of malpractice suits, bad patient outcomes, and concerns raised by colleagues. At the very core of this terrifying story — as with many similar examples — is the strong financial incentive for hospitals to hold on to their “superstar” surgeons given the high revenues they bring in. Awful awful awful.
- Here’s a great depiction of participant behavior at scientific meetings. Well done, Dr. Ilan Schwartz!
Extroverts and introverts at conferences https://t.co/c6lm45DjKv
— Ilan Schwartz MD PhD (@GermHunterMD) September 7, 2022
Seems particularly appropriate for us ID doctors, as we gradually return to in-person big public meetings.
- The rock group Blondie released a deluxe box set celebrating the years 1974-1982. In case you’re wondering about the inspiration for the photo at the top of this post, this classic album was released 44 years ago this month, became a prominent part of the soundtrack of my college years … and it wasn’t called Parallel Paws!
Anyway… the earworms all day have been Blondie so I'm going to listen to the first three albums back to back. Pure pop. They were the best singles band in the world for a couple of years there. Parallel lines is pretty much perfect. #FridayNightIsMusicNight pic.twitter.com/tg6eMvPK70
— anthony vickers (@untypicalboro) September 2, 2022
(Dog photo by Hollis Rafkin-Sax, edited by Anne Sax, based on a design idea by … me.)
2 Responses to “A Back To Work ID Link-o-Rama”

Paul E. Sax, MD
Contributing Editor
NEJM Journal Watch
Infectious Diseases
Biography | Disclosures | Summaries
Learn more about HIV and ID Observations.
 NEJM Journal Watch — Recent Infectious Disease Articles
NEJM Journal Watch — Recent Infectious Disease Articles- Observations from ID and Beyond: Hot Takes from IDWeek: CDC, COVID, and Two Doses of Dalbavancin
- Frailty Predicts Outcomes in Resistant Klebsiella pneumoniae Bacteremia
- Should Recipients of Kidney Transplants Receive Treatment for Asymptomatic Bacteriuria?
- COVID-19 mRNA Vaccines Aid Immune Checkpoint Inhibitor Cancer Therapy
- Cefiderocol in Health Care–Associated Gram-Negative Bacteremia
Hooray for the return of ID Link-o-Ramas! And that dog video made me laugh out loud.
Fantastic links and summaries- thanks! I am definitely intrigued by the small metformin signal in that trial, although I note that all patients in that trial were overweight. How much of the efficacy could possibly be attributed to metformin-induced improved blood glucose control in a patient group that likely contains some undiagnosed individuals with diabetes or prediabetes? I wonder whether metformin might be disproportionately effective such a group in ways that would not be useful in, say, a thin immunocompromised patient.