
An ongoing dialogue on HIV/AIDS, infectious diseases,
April 27th, 2014
Why ID/HIV Specialists Rank Last in MD Salaries
Here’s a figure from Medscape listing 2013 physician compensation:
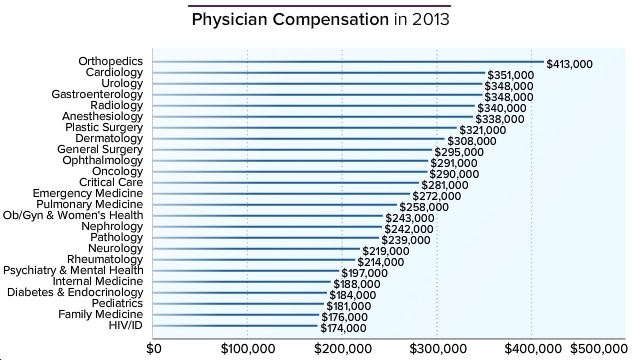
Now a median of $174,000/year is hardly chump change, so I don’t expect much in the way of sympathy on these data. On the other hand, someone has to to be last, and note that our income hasn’t increased a bit since the last time I commented on this survey three years ago.
So it’s worth taking a few moments listing the top reasons why we rank so low, most of them probably as obvious to you as the antibiotic of choice for treatment of syphilis. Then we’ll once again end on a happier note.
Reason #1: Doctors in the USA are paid the most for doing procedures. A famous ID doctor once said, “No one ever got rich from doing a gram stain.” And even though I just made that quote up, it’s definitely true. We ID doctors barely do any procedures, and the few we can do are comparatively low ticket items such as PAP smears, CSF exams, minor wound care, I and D, etc.
Some ID/HIV specialists have added various procedures to their practice to offset this deficit, such as screening for anal dysplasia in their HIV positive patients using high resolution anoscopy, doing fecal microbiota transplants for C diff, or providing injections of facial fillers for lipoatrophy — that last one most certainly a cash business. However, these enterprising (and for the first two, strong-stomached) ID docs are the exception, not the rule.
Reason #2: Productivity of doctors is still measured in volume. In a fee-for-service, count-the-RVUs system, the more patients you see the more you get paid. And I suspect there are few patients less amenable to high volume service than those referred to ID/HIV doctors.
Consider these: Fever of unknown origin (clinic or hospital/ICU setting). Spinal osteomyelitis/epidural abscess. New HIV diagnosis (especially with advanced disease/complications). Acute endocarditis. Lyme disease (real or imagined). Recurrent UTIs in patients with GU anatomic abnormalities or spinal cord injury. Fever in the returning traveler. Non-tuberculous mycobacterial lung infection. Infectious complication following major surgery. Tuberculosis of any sort. Sexually transmitted infections. Transplant-related infections. And on and on and on …
Reason #3: Many of the time-consuming services ID doctors provide have no billing code. Which means, simply, you can’t charge for your work. Did you spend an hour searching for a critical culture result done at an outside hospital? Maybe it was the orthopedics consult on a patient with a septic hip, now in your hospital with essentially zero information in the chart. And once this patient is treated, who’s going to arrange his/her post-discharge IV antibiotics? The lab test follow-up? The vancomycin levels?
That’s right, it’s you, Dr. Bugsndrugs, and not Dr. Breakbone who can bill plenty for the time in the OR, while you can only hope your documentation on the initial consult note meets appropriate complexity criteria for a C4 or C5. (Don’t forget the review of systems.) The rest of the work listed above (aside from that first note) is essentially gratis. On a different case, did you spend an eternity searching for the resistance genotype done in 1999, relegated to the proverbial dust heap — but now it’s absolutely crucial to find it as you try to craft a new HIV regimen for a patient with significant side effects? What’s the billing code for that? And don’t get me started on curbside consults and other informal advice to colleagues — just read this.
There are certainly other reasons for the low salary: low income means you can’t invest in money-making imaging/scanners (just a few have a FibroScan), there’s no ID-drug equivalent to Lucentis, a high proportion of us work on salary for a hospital/clinic rather than in private practice, and many participate in infection control/quality improvement programs that earn points for citizenship but rarely salary.
Yet despite the low revenue, we still seem to be doing great with two key questions — if we had to do it all over again, would we:
1) Choose to go into medicine [that is, still become a doctor]?
2) Choose the same specialty?
Here, low-ish revenues notwithstanding, we do pretty darn well, finishing second among specialties in question #1, and eighth in question #2. All of which means we’re pretty satisfied with our jobs — hardly surprising given that we have the privilege of working in such an interesting field. Money isn’t everything.
Take it away, boys!
16 Responses to “Why ID/HIV Specialists Rank Last in MD Salaries”

Paul E. Sax, MD
Contributing Editor
NEJM Journal Watch
Infectious Diseases
Biography | Disclosures | Summaries
Learn more about HIV and ID Observations.
 NEJM Journal Watch — Recent Infectious Disease Articles
NEJM Journal Watch — Recent Infectious Disease Articles- Diphtheria Outbreak in the EU: Reason for Concern
- First-Line Therapy for C. difficile Colitis: Does Fecal Microbiota Transplantation Have a Role?
- Observations from ID and Beyond: The Mystery of the Isolated Hepatitis B Core Antibody, Solved
- Observations from ID and Beyond: Federal HIV Guidelines Face a Shutdown — A Critical Loss for Clinicians and Patients
- Ceftriaxone for Patients Hospitalized with Pneumonia: One Gram or Two?
I am concerned about the validity of this data – ID/HIV had a 0% response rate!
Chris, I checked with Medscape — ID/HIV represented 0.5% of those who responded, not that 0.5% of HIV/ID docs who were asked responded to the survey. If you look at slide #30, you’ll see that the total number of respondents was 24,075 physicians, so around 1200 of the respondents (0.5% of the total) were ID/HIV docs.
They should have rounded it up to 1%, which is planned.
Paul
While the explosion of procedural care in several specialties and the impact of HIV have rearranged the list a bit, an observation from 25-30 years ago is still mostly accurate:
1) Physicians responsible for continuous care for the whole patient are paid least. (Primary care, in general)
2) Physicians who provide care either for a short time (ED, ICU, Surgery) or for a piece of the patient (single organ system) get paid more.
3) Physicians who have the least responsibility for the whole patient, or who never see the patient (…in the past, the “concessionaires” of radiology & laboratory) will be paid most.
I also wonder about the data, if no HIV/ID specialists responded to the survey.
Beyond that, I work in primary care and most of what Paul said applies to us as well. We spend about half our time doing things that are completely uncompensated (according to another survey/article referenced in the Medscape salary survey). My pet peeve is surgeons — yeah, I’m looking at *you*, Dr. Breakbone — who tell their patients to bring their disability paperwork to their PCP to be filled-out! Wait. You did the surgery that caused my patient to be temporarily disabled, but I am supposed to fill-out their disability paperwork? And when I tell my patients to call Dr. Breakbone’s office about the paperwork, they come back a week later and report, “No one will call me back”.
End of rant. And yes, I do still love primary care for a zillion reasons.
I sometimes feel guilty when I send patients to ID, for precisely the reasons Paul mentioned above. I know the ID doc is going to have to spend countless hours reviewing the patient’s history, reviewing old labs, ordering and interpreting new labs and just generally doing deep thinking. For this, they get to bill for a 99204 and not much else. The patients are often those for whom we in primary care are out of ideas, and we hope ID can somehow puzzle things out. And then, on top of everything, this amazing, detailed consult note comes back and I learn something new. All of which makes me, a nerd, sometimes wish I worked in ID. 🙂
As a Family Physician and Pediatrician who spent 5 years in 2 residencies, I see that my colleagues in both groups and almost at the bottom of the earnings barrel. The reasons for this are as mentioned. However, I enjoy continuity of cearning are and have had the privilege of taking care of 3 generations of families, including the children and grandchildren of some patients I delivered back when I did some obstetrics. At least one Dr. Breakbone in my communiity earns almost 10 times what I do, so I don’t cry any crocodile tears for orthopedic surgeons who complain about how unhappy they are with medicine. If I recall the Medscape survey correctly, they were #1 in unhappiness with medicine as a profession. I would like to see them go into another field where they can earn as much. I don’t think there are that many corporate CEO or Wall Street Banker/Stockbroker positions to go around.
To all the ID specialists out there: THANK YOU for the last 30 years of curbside consults you have given me. You are the most intellectual bunch out there and ALWAYS I learn so much from our interactions. It is actually criminal that you are the backbone of support to make us shine and keep us out of hot water, ie keep our patients from our non-ID docs guessing which antibiotic to give or not, but get paid the least.
Great article…save one feature. You could have written the same article, tweaking some of the examples, for geriatrics. It could be argued that we get paid even less. Notice Medscape doesn’t even acknowledge us….sad state of affairs given the “silver tsunami” everyone likes to reference and all geriatricians find abhorrent.
Agree with the geriatrician above. I am triple boarded in Family Practice, Geriatrics, Hospice and Palliative Care and the last two were not even included. We are under appreciated and undervalued.
It is obvious that cognitive endeavors seem to be the least remunerated. Either we need more clout vis-a-vis our input with the payers or perhaps we should all be paid the same on an hourly rate with offsets for years of training, malpractice costs and longevity due to burnout. Our commitment to our colleagues will not only be cudos for a job well done, but we would show monetarily our appreciation and support. We need all generalists and specialists to care for complexities of care that transcend the knowledge of even the most gifted clinician/surgeon. We should be able to practice the kind of medicine that we hold dear and not be held hostage to reimbursement inequities, debt, malpractice or the celebrity status of high wage earning physicians. Let’s hope the younger physicians will find a life balance more conducive to happiness than pay inequality or envy.
Have you guys ever heard of billing based on time in counseling? If you spend 60 minutes with a new patient and spend more than 50% of the time on counseling (on the data you dug up, on the results of the gram stain, of the choices of which anti-viral/abx are needed etc. etc.) then you can bill a 99205. You just have to be good at documenting this (and of course actually spend the time). It amazes me how much time and dedication some docs put into their work, spend the time with the patient painstakingly educating, then call the whole thing a 99203 or 204 because “r/o lyme disease” isn’t “technically” THAT complicated. Throwing money out the door.
0.5% of 24,075 would be around 120. I guess its a typo… the genius of Paul Sax is excused 🙂
The President of IDSA asks, “What’s keeping young people from choosing ID”? (http://news.idsociety.org/idsa/issues/2014-04-29/14.html) I think this graphic may have something to do with it. How many young people will choose to train an additional 2-4 years beyond Internal Medicine residency just to make less money and often work longer hours than their hospitalist colleagues? Fortunately, most people who make that decision against all financial logic, do it because they truly love the field of Infectious Diseases (and thus, HIV/ID scores highly on overall career satisfaction in the Medscape survey).
ID is still so much fun though! There are many aspects of my ID work that I would do for free (eg working up a fever in a tropical traveller, getting an SVR in a cirrhotic patient with HCV). Another important reason why I would “choose the same specialty again” is my colleagues – when one works in a unit where the emphasis is on bizarre diagnoses, exotic travel locations and nerdy discussions on plate rounds rather than cash generation and the next model of BMW, an intangible but exceptionally high value element is added to make this specialty a vocation not a profession.
Overall I’m pretty happy with my career choice as an ID specialist. I can’t be the bigger person however and sneer at the surgeons when they look at us and say: oh ! Here’s the infection “control” team !!!!! They can’t even tell the difference between infectious diseases and infection control ! That’s a bit much even for a surgeon :p
Sarah
Great post, Paul! While watching some other doctors spend far less time/effort and make far more money occasionally gives me indigestion, but when all is said and done, I believe the majority of us in ID are adequately compensated and quite satisfied knowing that our patients are getting solid medical care.
When I told a colleague of mine I wanted to go into ID, his answer was “Why would you do that? You end up doing the thinking for everyone else while they get paid and you don’t.” ID in a nutshell.