
An ongoing dialogue on HIV/AIDS, infectious diseases,
August 9th, 2020
Rapid Home Testing for Contagious COVID-19: How to Make It Happen
You know that feeling when you have an aha moment.
If you’re not familiar with the phrase, we can’t do better than our friends from Merriam-Webster:
aha moment (noun): a moment of sudden realization, inspiration, insight, recognition, or comprehension
This is how I felt when research revealed three key findings related to COVID-19 transmission:
- A small number of people account for a large number of cases. The handy estimate is that only 10-20% of people account for transmission of 80% of cases — it’s called “over-dispersion,” and is one important way that COVID-19 differs from influenza.
- “Superspreader” events happen when a person who has a high amount of virus comes in contact with a crowd or crowds. These events are far more likely to occur in indoor spaces with poor ventilation — hence the critical need for masking indoors. A pre-print server just posted an excellent study modeling these events, appropriately entitled, “Wrong person, place and time”.
- People may be highly contagious without knowing it. This is particularly true in the day before symptoms occur, the dreaded “pre-symptomatic” period. No amount of counseling or symptom screening or temperature sensing or other infection control theater can prevent pre-symptomatic people from mingling with others.
If we want to explain how this virus caused the largest global pandemic in over a century, those three facts will do just fine.
Which means that before we have an effective vaccine, the only thing that will help us interact safely with others is to test, test, and test some more — even when we don’t have symptoms.
A test you can do at home. Simply. Cheaply. With rapid turnaround time (15-30 minutes), actionable that day. Done as easy (and as frequently) as making a cup of coffee. (Metaphor chosen intentionally. Stay tuned.)
Plus, the test will correlate with what we need to know — how likely am I to spread the virus to another person? Can we open schools? Bars and restaurants? Start having concerts? Business and scientific conferences? Go to barbers and hair salons? Safely triage patients? Screen people in nursing homes, homeless shelters, prisons?
So while I might feel a bit guilty about posting yet again on this topic — really? can’t he think of anything else? — judging from the popularity of posts on this topic, I’m not alone with this obsession:
 Hey, one of the very best things about writing this blog over the years has been the intelligent comments from the community of readers — who are some of the smartest, most generous people out there since they’re reading an ID blog and providing such insight.
Hey, one of the very best things about writing this blog over the years has been the intelligent comments from the community of readers — who are some of the smartest, most generous people out there since they’re reading an ID blog and providing such insight.
And this one was particularly astute after my last post on this topic, from Dr. Anna Goldman:
Could the home test be marketed as a test of “contagious COVID,” instead of a straight COVID test? Maybe this reframing could help regulators and the public stop worrying about the comparison to the PCR test?
This, of course, gets right to the heart of the problem. We don’t have these tests yet because the regulators and others worry about lack of sensitivity.
But as noted multiple times, we do not need these tests to detect any tiny trace of the virus. We need them to be positive when a person has virus levels thousands or even millions of times higher than the lowest threshold of PCR positivity. When they’re most contagious. These will be tests for “contagious COVID!” Brilliant!
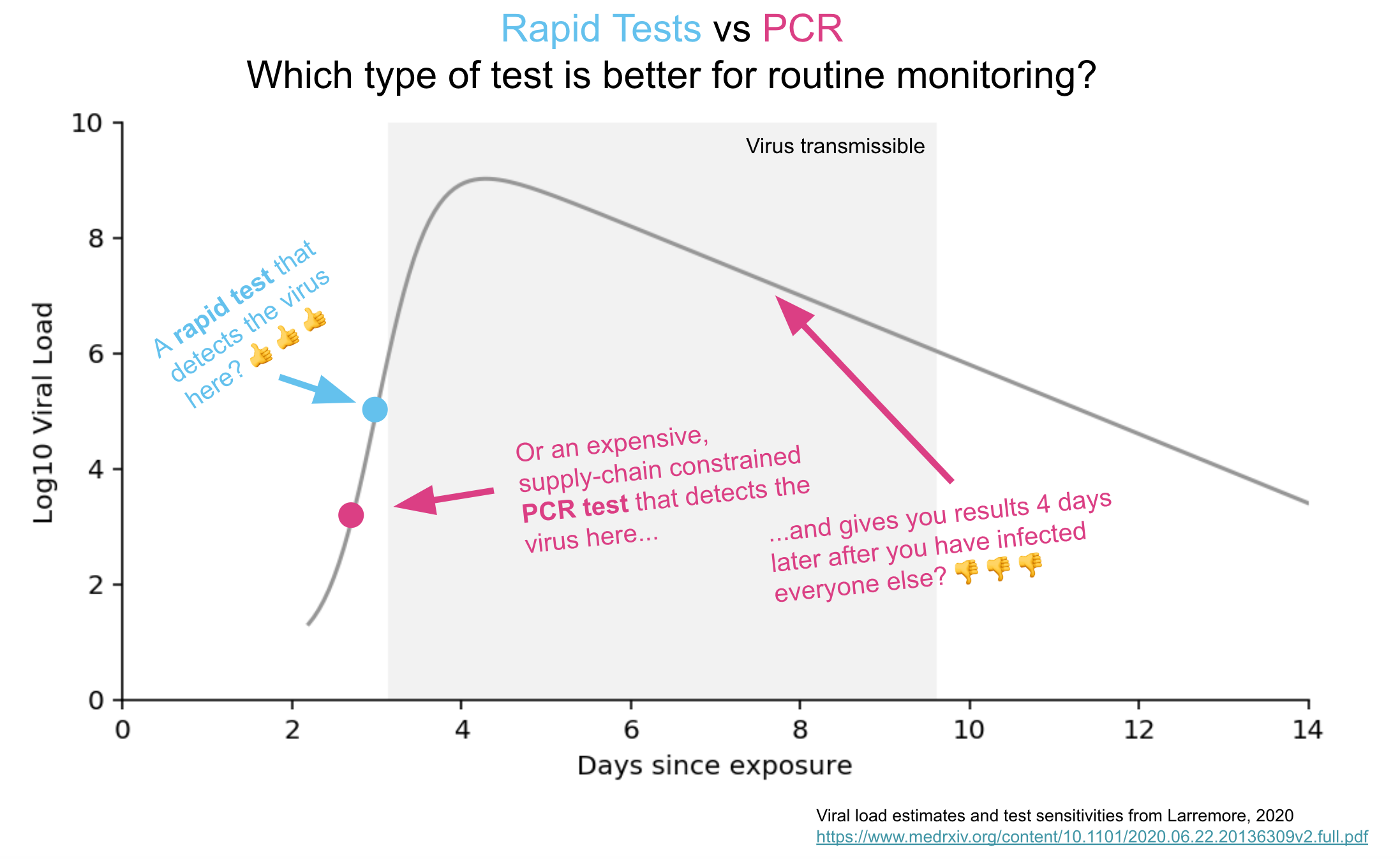
Figure courtesy of Chris Said.
Want further reassurance? As our old friend Thomas Bayes taught us, in the theorem that bears his name, when the prior probability of infection is low — as in the case of screening asymptomatic people in low incidence regions — the negative predictive value of even a test with imperfect sensitivity is high.
(In fact, we worry much more about false-positives and low positive predictive values with this strategy. But that’s a different hurdle.)
Now, I’ve written and talked and tweeted and done whatever I could to advocate for rapid home testing over the last month — I’m practically ready to hire a sky writer.
But even better, Chris Said (who runs the site rapidtests.org) has set up an easy way to contact our Senators, Representatives, and Governors. Do it now! Or give him some advice on memes, if you’re a meme-expert.
And, if there are any doubters out there, here’s another video featuring Dr. Michael Mina, an early and persuasive champion of this approach — and this one is only 5 minutes long.
Plus, you’ll understand why I chose the coffee metaphor.
Most important comment on youtube after this video?
This one:
I took the PCR test on July 22. Still haven’t received the results and it’s August 8. Totally. Stupid. I live in SF so maybe it’s better elsewhere but who cares what I was 17 days ago??
#RapidTestsNow
25 Responses to “Rapid Home Testing for Contagious COVID-19: How to Make It Happen”

Paul E. Sax, MD
Contributing Editor
NEJM Journal Watch
Infectious Diseases
Biography | Disclosures | Summaries
Learn more about HIV and ID Observations.
Thanks for your advocacy Paul. Sensitivity and specificity for these tests have been benchmarked against the presence of viral RNA rather than to live virus. If we were to do the latter, the performance of the rapid home paper tests or other similar such assays would likely appear better than PCR.
My assertion is that we need to infect as many low risk people as possible in the shortest amount of time to approach heard immunity. And bar for vaccine approval is 50% effectiveness. A recent survey said that only 34% of people would take the vaccine. Doing the math (I know, math is hard ), And taking people at their word (often a risky proposition), that means only 17% of the population get protected with the vaccine (and for how long). Even taking an optimistic guess and vaccine effectiveness of 66% only get you to roughly 22% with a 34% compliance with vaccination.
I know people blow smoke about not being sure that the illness confers immunity , but with essentially one strain circulating worldwide, it would be a very unusual situation for a natural infection with this virus not to confer strong, lifelong immunity, as with measles, mumps, any one strain of polio, varicella, etc. etc. natural infection will certainly be more protective than any vaccine developed, especially on the first go around.
I say (and I am 69 years old, have hypertension, atrial fibrillation moderate persistent asthma, and hereditary hemachromatosis) infect the young and the healthy, and the brave; isolate the sick, the old, and especially the old and sick, as well as the faint of heart camera and get this pandemic over with. Kind of like the pre-vaccination approach to chickenpox. Our kids are of an age, and they were chickenpox parties, or people took their kids over to the house of the newest case of chickenpox, so that The kids would get chickenpox while they were young and it was a relatively mild illness, and that when they were pre-adolescence adolescence, or God for bid, pregnant women. We knew chickenpox was inevitable, and we wanted to get it over with for her kids with the lowest risk of severe disease and complications.
The more that we know about this virus, now that the CCP has verdantly or in advertently released this on the world, it will be with us until heard immunity extinguishers it. And my calculations have just demonstrated if the vaccine is a shibboleth and or a unicorn.
But what the hell do I know? I’m just an old Family doc.
Well, I have practiced in Titan medicine in eight countries on four continents over 40 years. I have seen smallpox Go and AIDS come and become HIV; I have seen more vaccine preventable illness and physicians half my age, and I have seen vaccine recommendations go from one lifelong injection, to you need a booster; Polio go from injectable to oral to back to injectable; rotavirus vaccine come and go, Lyme vaccine come and go.
I may be old, but I’m not stupid.
Brilliant! I will repost this to support, as well as follow the links to contact my representatives. Thanks!
As doc working on covid outbreak management in a county health department, now a days we get most tests back in 48 hours (not so in April),but site contact testing is done 24 to 48 hours and often longer after the initial case is identified. We manage outbreaks fairly well, but the delays are maddening. The rapid test you describe (as I am sure you are well aware) would be a substantial improvement in public health pandemic management. It is long over due because of the regulatory and academic demand for high sensitivity and a disregard for practicality.
Paul the video link is not working
Reminiscent of the “Know your status” campaigns for HIV prevention, right? It’s a super important strategy .
However my brain went to the amount of resources needed (swabs/kits/packaging) for millions of people to test frequently….and the environmental waste that will create.
Oh dear – I get a message that the video has been removed from youtube, coffee notwithstanding
I’ve been on board with this and have been promoting the cause even on our local TV station. Thanks for the suggestions.
Perhaps while we are at we should make some noise about the proposed FOUR PERCENT DECREASE – yes decrease – in Infectious Disease doctors Medicare 2021 fees. Why are we not a winner like our other cognitive colleagues: endocrinology (17%), rheumatology (16%), hematology/oncology (14%)? Why are we one of the three medicine losers: dermatology -2% and gastroenterology -5%? Even cardiology got a 1% increase! Are we considered a surgical specialty because we can actually cure people of some of their diseases? For more information, go to page 897 in the CMS proposed ruling.
I was hoping with COVID our specialty would finally get the recognition it deserved. Once again, we are so busy helping others we are missing the ball on this one. COVID might end up putting the nail in our own coffins.
As I said before : http://pregnancyfeet.site
So…. I’m already convinced. I’m the owner of a small medical practice in Maine. How can I get started now? Are there any sources available now?
Enthusiastically, Scott Schiff-Slater MD
always appreciate your posts and share these covid-related especially. A friend of mine (DMD) likes to post skeptical replies such as (https://sebastianrushworth.com/2020/08/04/how-bad-is-covid-really-a-swedish-doctors-perspective/?fbclid=IwAR0VuCeh_sAiCHugmxo5YQ-Jc6aPT-X59-zhKIvsjtYU0afGFjGAK9EkYaE), I would love to hear your responses to some of the more articulate criticisms.
Fantastic Paul. I have already started sent out your editorial to dozens of people, hundreds of patients, family and friends – AND – included the website – http://www.RapidTests.org. Let’ do this!!
This could be a valuable tool, but we should not confuse it with a magic bullet. The limitation on its impact will probably not be the limited sensitivity, but our usual biggest problem … us.
This outbreak has disproportionately impacted underserved communities, which often have lower health literacy. While the idea of doing this test appeals to doctors and people who read every page of the NY Times or the Wall Street Journal, we may see more limited uptake in communities with less access to health information and health care. And even if they get the test and do it, what will they do with the information? Will people who live in a 2-bedroom apartment with 8 others, and have no paid sick leave, be able to isolate themselves and stay home from work? Given the number of doctors who come to work with the flu, we should not be too quick to condemn people who don’t respond appropriately to the test results, wrong as it may be.
Furthermore, the politicization of the outbreak and the continued spread of misinformation continue to hobble us. Will people who “don’t believe in masks” or “don’t believe in coronavirus” (are they talking about a virus or the Tooth Fairy) do this test? Will leaders who have tried to suppress testing endorse this approach for their followers?
These issues will have to be addressed if this approach to testing is to have the hoped-for impact at a population level.
The good news is- such a test is already available. The rapid antigen test- The test isnt too sensitive compared to an RT-PCR. However has been shown to be positive in those with higher viral loads- roughly with Ct values of 25 or below, while being highly specific. The only downside is the requirement of a nasopharyngeal swab which may be difficult to self-collect. But a good quantity of saliva would be an excellent alternative, if the test is made adaptable for this specimen- saliva was shown to be almost as good as an NP swab by To et al in an earlier Lancet paper.
Ok I saw the video after posting the comment- redundant!
Paul
can you get this information to Tony Fauci? This makes so much sense. something our political leaders are lacking.
I second that. Paul must be able to contact Fauci. As a physician I get the initial reluctance to accept a less sensitive test. However if used as a public health screening tool and we target infectious Covid with cheap, frequent testing it will work. At some level what we need is a good enough “magic bullet” to gain control of the highly emotional fear factor that is ruining economies and lives. This looks to me like just such a magic bullet.
Definitely agree, we need home base rapid test.
And what about oral effective treatment that is widely available and so infected patient and house hold plus close contacts through PCP’s office and urgent care before they get into Cytokine storm and inflammatory cascade. Lately vaccine rates are low even for regular childhood recommended vaccine.
We also need push on oral effective widely available treatment.
Excellent piece, as always. My question is, what is the False Positive rate of these tests? In many was I think this is much more important than the False Negative rate for getting the public, especially the doubters, to accept such a test. What happens when someone gets a False positive result and then goes through the hassle of staying home, missing paycheck, important event, etc… only to find out it was unnecessary and then posts about it in social media? The doubters have a field day and then we are in the same situation we are now with getting people to wear masks. I love the idea, but I think a super low false positive rate will be needed to get public acceptance.
Good afternoon
Thank Dr. Roger Kimber for his great common sense in supporting the development of herd immunity concurrently with shielding populations at risk of severe COVID-19. It is also very remarkable the disclosure of the sensible application of rapid saliva tests that Dr. Paul Sax has carried out.
Everything is so reasonable that its global ignorance is painful.
Brilliant… Let’s go
Hi Paul,
Thank you for championing this cause, with which I agree. It was heartening to hear Joe Biden prioritize broad access to rapid testing in his convention speech, but I hope we don’t have to wait until next year!
Kimon
Your dog is going to wish all kinds of stuff in his new home.
Luckily, there are a lot of steps you’ll be able to take to easy the
transition.
I recency ordered antibody from tests from EDM great service and products. http://www.emdintl.com