
An ongoing dialogue on HIV/AIDS, infectious diseases,
August 2nd, 2021
Provincetown July Celebration a Challenging Stress Test for the COVID-19 Vaccines
When the complete history of the COVID-19 pandemic is eventually written — and boy oh boy, can’t wait for that — certain events will feature prominently as sites of notable outbreaks.
The Diamond Princess cruise ship
The Biogen Leadership conference
The Skagit Valley Chorale practice
The Amy Coney Barrett White House reception
And now:
The Provincetown Independence Week celebration
So what sets the last one apart from the others? And why did it lead to a change in CDC guidance about masking indoors for vaccinated people?
The answer to question #1 is, of course, that the other events occurred before we had effective vaccines and the highly transmissible Delta variant.
But what about question #2? Why the reversal on masking indoors for people who have been vaccinated?
In addition to the sheer number of cases that occurred in vaccinated people, here’s the primary reason, in graphic form from MMWR: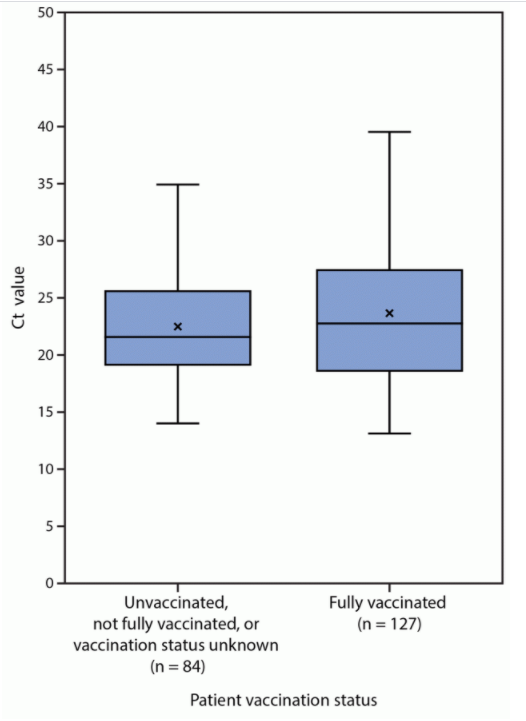
The vertical axis is the cycle threshold value, a measure of how much virus is in the sample (lower is more virus). And as is plainly evident, these results are similar for vaccinated and unvaccinated people.
These suggest that vaccinated people with COVID-19 could spread the virus to others as easily as unvaccinated people. It’s not proof, as it discounts the immune response, which may dampen contagious virus and shorten the duration of viral shedding.
It’s also in contrast with other studies that do show lower viral burdens over time in people who have been vaccinated — including this highly relevant recent study from Singapore:
A recent study out of Singapore shows not only does vaccination prevent you from getting sick with Delta (B.1.617.2), but it is associated with faster decline in viral RNA load. What does this mean? Vaccines make you LESS infectious!
— Chise (@sailorrooscout) July 31, 2021
Regardless, it underscores the plain fact that anyone with symptoms consistent with COVID-19 needs to isolate until recovery, vaccination status notwithstanding. For those diagnosed, we may even need to institute different isolation protocols, since the higher viral loads seen with Delta could mean more transmissions further out from onset of symptoms.
Already, the CDC has recommended that vaccinated people exposed to COVID-19 should get tested afterward, a return to pre-vaccine guidance. Should we also recommend antigen testing in breakthrough cases before return to work? (PCR may continue to detect non-viable viral fragments long beyond the contagious phase.)
What the outbreak can’t tell us is how bad this would have been without vaccines at all. Yes, there were lots of cases, but so far relatively few hospitalizations, and no deaths. Yikes, the mind boggles.
Because if anyone is under the impression that Provincetown is the kind of sleepy Cape Cod small town made famous through Edward Hopper’s dreamy artwork, think again — this July celebration is the diametric opposite. All who attended reported plenty of crowded bars, restaurants, and dance parties, with many shared accommodations among travelers.
You could hardly imagine a better environment for SARS-CoV-2 transmission. These settings plus the Delta variant provided the ultimate stress test for the vaccines.
What the outbreak also can’t tell us is how commonly asymptomatic people who are vaccinated acquire SARS-CoV-2 and then transmit it onward. This question has been filling up the email inboxes of every ID specialist out there.
I suspect it’s uncommon. But let’s not be overconfident about anything related to this tricky virus, which has bedeviled us with unpredictable twists and turns from the start. Humility!
This is quite the figure, from a @CDCgov presentation.
Further evidence of the critical role of humility when it comes to predicting what's next in this pandemic, a lesson we all need to learn again and again.
H/T @washingtonpost https://t.co/1LnqGojF3V pic.twitter.com/IlymSsJOOX
— Paul Sax (@PaulSaxMD) July 30, 2021
Yes, that’s a scary figure. What to do in the meantime as Delta is surging?
Get as many eligible people vaccinated as possible. Remember, the vaccines reduce transmission risk in two ways:
- Decreasing the probability of infection in the first place, either symptomatic or asymptomatic
- Decreasing the duration of infectiousness for those who do get infected
That first effect is ironclad — no virus, no transmission. The second one is a bonus. The evidence is strong that both of these are in play with COVID-19 vaccines, as summarized in this superb review.
So approve the vaccines already, FDA! This will allow broader implementation of vaccine mandates in schools and workplaces.
Plus, when possible, we should limit socializing indoors to gatherings with other vaccinated people. Since not everyone can be vaccinated — kids under 12, for example — if you’re planning a large indoor event, go ahead and ask people to get tested ahead of time. We might ask even if everyone is vaccinated, especially if the event has immunocompromised guests. Good tests are widely available over the counter that can give results back in 15 minutes. Let’s use them!
And whatever is causing COVID-19 case numbers to decline rapidly in the United Kingdom and India, here’s hoping it happens here as well.
11 Responses to “Provincetown July Celebration a Challenging Stress Test for the COVID-19 Vaccines”

Paul E. Sax, MD
Contributing Editor
NEJM Journal Watch
Infectious Diseases
Biography | Disclosures | Summaries
Learn more about HIV and ID Observations.
As the CDC and other public health leaders revert back to broad non-pharma interventions like universal masking, I’m wondering what our endgame is here. This virus is almost certainly never going to be eradicated. The Delta variant is obviously bad news, but our vaccines seem to be highly protective against bad outcomes for the small fraction of breakthrough cases. Anyone unvaccinated at this point is almost certainly putting themselves at risk by choice – we should keep reaching out to them (and mandating vaccination as much as feasible), but I don’t want to put my life on hold for them indefinitely. Maybe it’s time to just let Delta rip through the vaccinated population and provide a natural booster before the next (vaccine-resistant) variant comes along. Yes, we need to protect the immunocompromised and extreme elderly and others for whom vaccine efficacy may be a question, but what are the trade offs here?
Paul, what do you make of the Ct values in the Provincetown cohort when compared to those reported earlier in the CDC briefing slides?
For example:
Breakthrough cases reported to national passive surveillance have lower Ct values by 3 cycles (~10-fold increase in viral load) for Delta (Ct=18, n=19) compared with Alpha (Ct=21, n=207) and other lineages (Ct=21, n=251).
In Barnstable County, MA, outbreak: there was no difference in mean Ct values in vaccinated and unvaccinated cases [median among vaccinated (n=80): 21.9; unvaccinated (n=65): 21.5]
I’m not sure how much these values can be compared across platforms, but as ithat seems to be what the CDC is doing here, doesn’t this suggest some degree of attenuation of infection with delta in both the vaccinated and unvaccinated cohorts?
Small numbers but it seems as if this is hypothesis generating on multiple levels.
Excellent summation
Also loved the Edward Hopper comment.
How does this compare with other diseases? It seems a lot of vaccinated people are getting tested with no or minimal symptoms? How often do we do that for influenza? When polio and measles vaccines came out was testing done on minimally sick patients? I know each disease is different but I am curious as we often compare effectiveness rates of the different vaccines and I wonder if it’s a fair comparison.
In all the media reports regarding the Provincetown outbreak of Delta variant SARS-CoV-2 it was not reported which vaccine had been administered to those positive for COVID despite vaccination. Might it have been that J&J vaccine had been administered to many of these infected individuals? The mRNA vaccines were available first and used primarily on the elderly and immunocompromised. Reports of the Provincetown outbreak also were devoid of immunocompromised states of individuals who may have been being treated for HIV also. As usual in these media reports details are missing.
RE: Margaret Pothier. Maybe news outlets didn’t give details of the vaccine products that these individuals had received, but the CDC’s MMWR issue did (MMWR are publicly available reports that the CDC publishes, on outbreaks and such).
“Among the 469 cases in Massachusetts residents, 346 (74%) occurred in persons who were fully vaccinated; of these, 301 (87%) were male, with a median age of 42 years. Vaccine products received by persons experiencing breakthrough infections were Pfizer-BioNTech (159; 46%), Moderna (131; 38%), and Janssen (56; 16%);”
Link: https://www.cdc.gov/mmwr/volumes/70/wr/mm7031e2.htm
Excellent points Margaret. Perhaps the unexpected rate of COVID infection in vaccinated individuals and the higher viral loads in the Provincetown cohort might correlate to the type of vaccine, however the cohort of vaccinated individuals in Provincetown may reflect a subset of individuals who are more at risk for HIV positive status than the general population, and who may be on maintenance antiretroviral medications or use PrEP. These characteristics possibly could have contributed to an increase risk of breakthrough infections and higher SARS CoV-2 viral loads.
As this outbreak is studied it would be helpful to ask the questions if factors such as HIV status, CD4 counts, and antiretroviral or PrEP therapy might have contributed to both breakthrough infection in vaccinated individuals and the measured higher than expected SARS CoV2 viral loads.
Like Provincetown, the Sturgis motorcycle rally will create an environment leading to a much higher rate of COVID-19 in vaccinated as well as unvaccinated individuals. It may be an opportunity, while unfortunate, to gather a lot of information on the delta variant’s infection rates in both vaccinated and unvaccinated individuals, viral loads, and clinical outcomes.
If you want more details, you can read the CDC’s public report (i.e. MMWR) about it: https://www.cdc.gov/mmwr/volumes/70/wr/mm7031e2.htm
“Among the 469 cases in Massachusetts residents, 346 (74%) occurred in persons who were fully vaccinated; of these, 301 (87%) were male, with a median age of 42 years. Vaccine products received by persons experiencing breakthrough infections were Pfizer-BioNTech (159; 46%), Moderna (131; 38%), and Janssen (56; 16%); among fully vaccinated persons in the Massachusetts general population, 56% had received Pfizer-BioNTech, 38% had received Moderna, and 7% had received Janssen vaccine products.”
I guess I’m upset with the lack of transparency on the Massachusetts event. Epidemiology is the key for understanding outbreaks and the information released through MMWR and news media has been sparse in explaining what was happening that weekend.
Based on an LATimes opinion piece from someone who attended: (https://www.google.com/amp/s/www.latimes.com/opinion/story/2021-08-04/lessons-on-covid-and-life-from-provincetowns-outbreak-of-normalcy%3f_amp=true). The initial 4th of July weekend had 60,000 attend a “Bear Weekend Bash”. It was Mardi Gras on steroids. The bars were overcrowded, tons of alcohol, in mostly (let’s face it, obese by BMI criteria) middle-aged men who had not had fun in 1.5 years! I calculate 60,000 potential exposed and less than 400 cases in the fully vaccinated. To me the vaccine did FANTASTIC in this environment and the rates of transmission were within what would be normally expected for the vaccine.
As far at the high viral titers in immunized folk—no mention if any were immunocompromised? Only thing mentioned was “2 of the immunized hospitalized group had underlying conditions”. What was/were the underlying condition(s). I think that would be important to know in an epidemiologic report.
I don’t believe this event can be extrapolated so easily.
The reports are also leaving out information on prior COVID infection. Massachusetts DPH has account of all positive cases and has been doing contact tracing for over a year now. I am sure it would be eye opening to see how many (if any!!) of these cases from the Provincetown cluster are reinfection. I am sure it would be easy enough to track in their database as they took the step to verify vaccine status in the MIIS registry. Why is this information not transparent?
Another clarifying and amusing blog post from Dr. Sax.
Keep them coming!