
An ongoing dialogue on HIV/AIDS, infectious diseases,
January 10th, 2016
Medical Marijuana and Painful Neuropathy — An Opportunity to Make Us Believers
 Medical marijuana is now officially available in New York, the city with by far the largest number of people living with HIV/AIDS in the country. Reporting on the first dispensary in Manhattan, the aptly named Julie Weed (yes! her real name!) writes:
Medical marijuana is now officially available in New York, the city with by far the largest number of people living with HIV/AIDS in the country. Reporting on the first dispensary in Manhattan, the aptly named Julie Weed (yes! her real name!) writes:
One of the most promising areas for research is the substitution of medical marijuana for opioids like OxyContin and Percocet for pain management …“68% of our patients with AIDS-related neuropathy have said that medical marijuana has allowed them to stop taking opioid prescription pain killers which can be addictive, cause a variety of harmful side-effects, and — most critically – are the cause of thousands of overdose deaths per year.”
Some thoughts based on this claim, and the long history of medical marijuana and HIV/AIDS:
- Could 68% of patients with painful peripheral neuropathy really stop opioid pain killers with marijuana? Wow. If that’s true, it’s huge — even half this rate would be a dramatic advance. Among the most frustrating conditions in all of medicine, painful peripheral neuropathy has a list of treatments as varied as the products sold in the “Cough and Cold” aisle at your pharmacy — and are, unfortunately, about equally effective. Proven strategies to help people come off chronic narcotics are badly needed.
- HIV specialists have been hearing about the medical use of marijuana even longer than we’ve had effective antiretroviral therapy. Initially touted as an appetite stimulant for HIV-related anorexia and weight loss, and as palliative therapy to ease the pain of death and dying, it gained further use in the mid-1990s when early HIV-related combination regimens caused so much nausea. This randomized clinical trial led by Donald Abrams — who has done some of the best work studying marijuana in HIV against great odds — found that 5 days of smoked cannabis was more effective than placebo in 50 patients with painful peripheral neuropathy. Of course blinding the study arms was (and remains) essentially impossible given the euphoric effects of the drug, but maybe that’s the whole point.
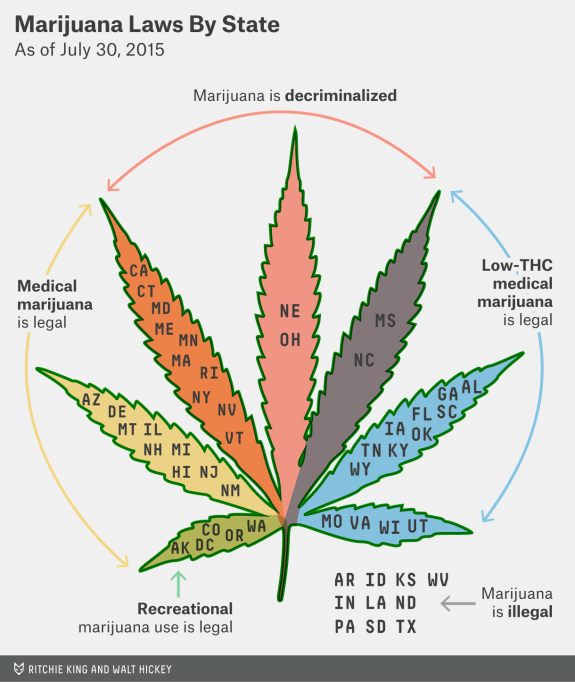
- Just legalize the stuff already. That’s how I’d characterize the opinion on marijuana for the vast majority of the doctors, nurses, and social workers I work with, some of whom (like me) both remember Woodstock (the original one, kids) and enjoy the music from it, or are younger, and have the same view. If marijuana is legalized, it can be more easily regulated, taxed, and studied (see below) — just like that other legal psychoactive drug, alcohol. Seems like this is hardly a minority view (the link is to the source of the graphic at the top of the page).
- Legalization would allow more rigorous studies of therapeutic use, long-term effects, and safety. Such studies are now essentially prohibited by the federal government since marijuana is considered a drug of abuse. As a result, many claims about its medical indications are based on either small, short term, or methodologically questionable studies or, even worse, strongly-held beliefs based mostly on anecdote — the weakest form of scientific evidence. That is, I’m afraid, what that “68% have stopped their opiates” claim is from the opening paragraph. Until it’s studied more rigorously, we’re stuck with the frustration of dealing with claims that marijuana is a valid treatment for practically every chronic condition under the sun. A similar claim might be made of benzodiazepines like Valium, Xanax, and Klonopin — which definitely make people feel better — but clinical research has more clearly defined both the benefits and risks of this drug class.
- The quasi-medical atmosphere of some marijuana dispensaries is a huge negative to the acceptance of legitimate medical use. Got a free 10 minutes? That plus saying you have “insomnia” gets you a weed license for the medical stuff in Venice, no medical records required. Medical marijuana exists in this bizarre parallel system to “real” FDA approved drugs, and the absence of good scientific data means that the indications for use state-by-state are literally and figuratively all over the map. Got to love this indication (and I use the word loosely) for medical use from California: “Any other chronic or persistent medical symptom that substantially limits the ability of the person to conduct one or more major life activities (as defined by the Americans with Disabilities Act of 1990) or, if not alleviated, may cause serious harm to the patient’s safety or physical or mental health.” If it’s based on patient report, that covers pretty much anything, doesn’t it?
So what’s my take right now? Count me in the same camp as these authors, who published their views in a JAMA editorial last year, writing:
If the states’ initiative to legalize medical marijuana is merely a veiled step toward allowing access to recreational marijuana, then the medical community should be left out of the process, and instead marijuana should be decriminalized … Evidence justifying marijuana use for various medical conditions will require the conduct of adequately powered, double-blind, randomized, placebo/active controlled clinical trials to test its short- and long-term efficacy and safety. The federal government and states should support medical marijuana research.
Totally agree. Meanwhile, here’s a study design free for the taking:
Title: A randomized, blinded study of cannabis versus placebo to reduce opiate use in HIV-related neuropathic pain.
Entry criteria: Painful HIV-related neuropathy for ≥3 months, confirmed by a neurologist at screening, and requiring the use of opiates for control. Stable doses of opiates for at least 4 weeks prior to screening are required. HIV RNA must be < 50 copies/mL on non-neurotoxic containing ART.
Intervention: Smoked cannabis or placebo for 24 weeks; up to daily use as desired by study subjects. Adjunctive therapies (gabapentin, antiepileptics, non-steroidal anti-inflammatory drugs, acupuncture) will be administered at the discretion of the investigators.
Primary endpoint: Time to cessation of opiate use as estimated by the Kaplan-Meier method.
Secondary endpoints: Time to reduction in 25, 50, and 75% of opiate use; absolute and relative reduction in opiate dose. Proportion opiate free at study completion. And what the hell, might as well also do Numeric Pain Rating Scale, Change in Pain Inventory Score, Numeric Rating Scale Sleep Interference Score, Medical Outcomes Study Sleep Scale, Patient Global Impression of Change of Pain, and all those other neuropathy assessments. Throw in some neurocognitive testing just for fun.
Funding: National Institutes of Health
You’re welcome!
Let’s see if what you think.
12 Responses to “Medical Marijuana and Painful Neuropathy — An Opportunity to Make Us Believers”

Paul E. Sax, MD
Contributing Editor
NEJM Journal Watch
Infectious Diseases
Biography | Disclosures | Summaries
Learn more about HIV and ID Observations.
The current situtaiton is absurd. In New Mexico we have medical marijuana. HIV infection qualifies you for a card, but as the patient’s physician I have to fill out and sign a two-page form stating that my patients are “disabled” as a result of their HIV infection. The alternative is that they have to buy it illegally, risking prosecution. I won’t put my approach to this dilemma in writing; I’ll let you guess what I do. Meanwhile, just a couple hours’ drive to the north, Colorado sells marijuana to anyone who wants it, and no one is searching their cars when they drive back across the border. New Mexico is poor, and Colorado is getting richer all the time. This has got to stop. It’s just a weed, for God’s sake!
It is quite hard to blind subjects on whether they are smoking marijuana or placebo
Marihuana can be applied topically and has NO systemic effects. It is easy to use the vehicle as a placebo
I would have THC at every corner store – if only we could have full disclosure – risks, benefits, side effects, etc. NOT like alcohol – would alcohol be released as a drug today if it had to qualify – 5% permanent fatal addiction used as directed!!!??? or cigarettes – 100% lethal used as directed????? It is not the “evil” weed – nor is it “just a weed” – it’s a potent potentially permanent brain changing chemical – if the Government gave that to us there would be outrage – oh oh, did someone say “opiate of the masses” . . .better stop now (or “get yelled at again”).
Does society really need another mind-altering substance? I have no problem with decriminalization and medical use of marijuana. But States are pursuing decriminalization not for altruistic reasons but because they lust for greater tax revenues. Inevitably, increased recreational marijuana use will diffuse to younger populations with likely deleterious neurological and behavioral effects.
There are abundant non-drug ways to get “high.” Would anyone consider: talking to a friend, listening to music, dancing, meditating, etc. Oh, right, there’s no tax money to be collected or profits to be made.
I feel that while there are clear harms from smoking marijuana (you can argue how benign they may be in comparison, but it’s not water), I think any discussion of this needs to account for the harms of criminalization which can prevent someone with a drug charge from obtaining federal student loans (and thus getting to college), getting a job, or having a equitable chance of escaping the cylce of poverty. I don’t think that criminalization is an proportionate response to marijuana. The medical question was already covered well by Paul.
Will will soon find out if the legalization of marijuana will have harmful effects on society as we study the results of legalization in Colorado and Washington State.
As a general family doc I have had excellent experience using topical marihuana (dissolved in olive oil) for peripheral neuropathy. It has been much more effective than the usual prescribed medications in usually, elderly, hesitant, and skeptical patients. It is effective in my experience in trigeminal neuralgia, post herpetic neuralgia, and diabetic peripheral neuropathy. In the later case the patient can test by treating one leg and not the other. Occasionally the allodynia is cured and ongoing RX is not necessary. My patients have not experienced mental or systemic side effects. It is disheartening that medicine is being forced by law and culture to overlook this very effective modality.
There is real medical marijuana available now in all US jurisdictions. It is called Marinol, aka dronabinol. 100% pure, not adulterated, known potency, etc.
People enamored of ‘medical marijuana’ are in large part pot heads or ex-pot heads in and out of the profession who are seeking slippery slope back door legalization. For physicians, especially those of the left who want to regulate e-cigarettes for God’s sake, is the height of hypocrisy and ignorance.
It would never be approved if it had to pass the usual FDA gauntlet.
Spare me the sob stories, and the anecdotal experiences. You people are not believable.
Marinol is mildly effective at improving appetite. At high but usually intolerable doses it may help to control nausea. In those who tolerate the sedation, I’ve never found it useful for anything else. You certainly don’t hear patients talk about pain control with Marinol, and I’ve never seen it allow patients to wean themselves off opiates, as I have with marijuana. Marinol is NOT marijuana.
I’m not “enamored” of medical marijuana, because I don’t think physicians should be put in the position of having to decide who needs it for medical reasons. I’m in favor of legalization.
How many of the respondents have inquired of their respective local experts in Addiction Medicine, e.g. on this? Coming from the pharma industry, working in 3 States on opiod-related matters, I was surprised when I became informed of their position on pot legalization. In a nutshell, its not “just pot”.
Alcohol, tobacco, car exhaust, sugar, big macs, some tap water, sodas, meat, sports, TV, Twitter, most workplaces, capitalism, are all far more dangerous than pot to body, mind, and soul, but we have somehow managed to live with them and even find enjoyment in them. If we could live for eternity I would argue to outlaw all of them, but we don’t, thank the gods. Legalize it already or lets bring back witch burning.