
An ongoing dialogue on HIV/AIDS, infectious diseases,
April 1st, 2022
As the World Around Us Moves On, We ID Docs Just … Can’t
Cheaper (and tastier) than ivermectin — and a whole car load!
Something quite remarkable happened as Omicron tore through the United States in December and January.
Despite triggering a record number of cases — which should have made people more concerned about COVID-19 — Omicron paradoxically did the opposite. It made most of our country decide to move on, even parts famous (or infamous, depending on your view) for being careful. Just to live with this COVID thing — ending vaccine mandates, leaving the masks at home, going back to restaurants, gyms, large parties.
Hey, I get it. When facing something so contagious, something that easily broke through our vaccines, something that even extremely cautious people ended up contracting, we might start having that “what’s the use?” feeling.
Time to get back to normal. Shrugs. Even as cases (and hospitalizations) increase in Western Europe, this relaxed attitude prevails, prompting Dr. Walid Gellad to wonder, Why is everyone so chill?
I’m convinced a major amplifier of this casual response is the reduced per-case clinical severity of Omicron, largely due to partial existing immunity from vaccination, prior infection, or both. This lower severity on an individual level means everyone knows — or experienced themselves — cases that were quite mild.
Typical statements uttered by patients, colleagues, friends, acquaintances during the Omicron surge:
“Felt like a cold.”
“If it weren’t for my positive rapid home test, I still would have come to work.”
“Had one day of feeling blah, then mostly it was lots of nasal congestion.”
“I can’t believe he [referring to a school-age kid] tested positive, he’s as active and energetic as ever.”
“You’ll never believe this, but she [referring to an older family member in a nursing home] tested positive, and we just got off a Zoom call — she seems fine!”
But here’s the problem — the denominator of cases was so ginormous during Omicron that it still led to a staggering number of hospitalizations and deaths. Way more than from flu, even in a bad flu year. People who had weakened immune systems, had multiple medical problems, were still unvaccinated, or were just unlucky to get a really bad case still experienced severe disease. And some fraction of all these Omicron cases will be left with long COVID, evaluation and treatment of which remains in its infancy.
Some people may not have seen this numerator. But believe me, we sure felt it, as did our hospitals. We still needed the ICU beds for some COVID patients, still adhered to strict infection prevention measures for everyone with a positive COVID test admitted to the hospital, still struggled to clear hospital workers (who came down with Omicron just as much as everyone else) for return to work.
You need no further evidence of how the Omicron surge disrupted patient care than to observe how many hospitals delayed non-essential surgeries. Not only is elective surgery important for good patient care (ask anyone who had their surgery delayed), but also this is the most remunerative service provided by most hospitals in the United States. As a result, I doubt there’s a single hospital in the country that didn’t have a negative balance sheet during Omicron.
Now, as we ID docs watch what happened in Western Europe, we can’t help but squirm. “What happens in the U.K. most certainly DOES NOT STAY in the U.K.” should be public health’s advertising slogan for what comes next in the northeastern USA:
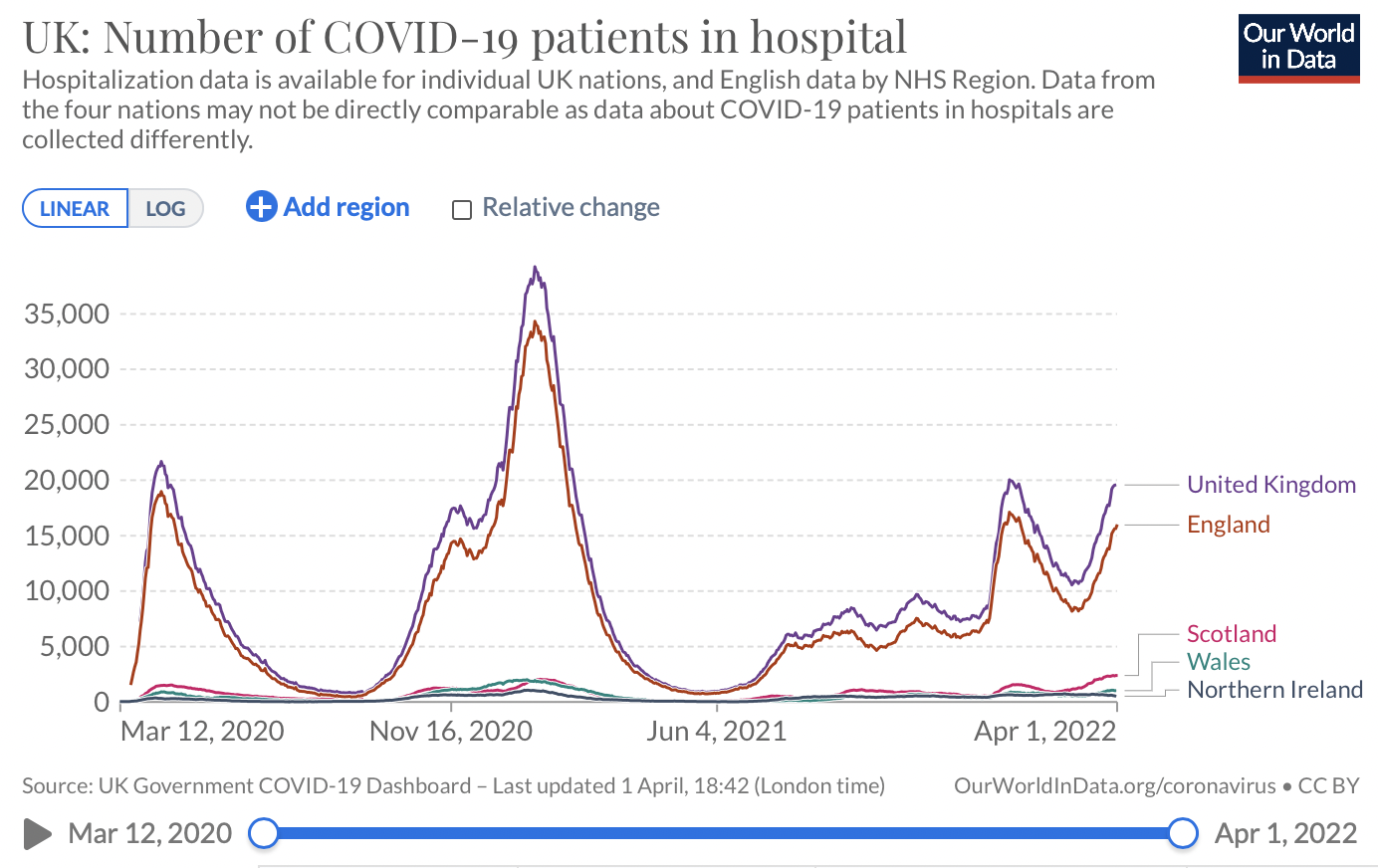
ourworldindata.org/grapher/uk-covid-hospital-patients
Already we see the trend starting, with the increase in wastewater concentrations of the virus in most regions, a rise in the reported test-positivity rate, and a slow creep up in people testing positive among those hospitalized. All this generates more calls about exposures in the workplace and at home, about how to get nirmatrelvir, about the latest monoclonal antibody taken down by viral evolution, and this week a zillion people asking about whether to get a booster now, wait until just before a fall surge, or wait for a variant-specific vaccine.
You know, the pandemic life of an ID doctor.
So while much of the rest of the population has moved on, forgive us ID docs if we remain nervous Nellies. We can hope that case numbers will be lower during the BA.2 Omicron surge — and they might be — but we can’t count on it.
Now, I just have to get that smell of onions out of my car …
27 Responses to “As the World Around Us Moves On, We ID Docs Just … Can’t”

Paul E. Sax, MD
Contributing Editor
NEJM Journal Watch
Infectious Diseases
Biography | Disclosures | Summaries
Learn more about HIV and ID Observations.
I am desperate for your wisdom on a 4th dose…The Israeli data on health care workers with or without a 4th dose is not encouraging-25% incidence of infection in those w 3 doses vs 18-20% incidence in those w 4 doses at 30 days. I agree with those who suggest maybe we need to rethink the current vaccines and consider a mucosal/intranasal version to hit Omicron where it enters the body, as the current vaccines don’t seem to offer durable additional protection. I would be very grateful for your thoughts as a healthy 58 year old who is schedule for a 4th dose on 4/6-about 6 months after my 3rd dose!
The vaccines only create neutralizing antibodies, specifically the S protein. This worked very effectively with the original variants until Omicron. It learned how to get around the S protein and since the N protein is not produced by the vaccine, that’s why fully vaccinated people contracted Omicron. The vaccine still afforded some protection but not fully. New vaccine will need to produce the different kinds of proteins to ensure protection against further variants…. That and the vast majority of the worlds population will need to be vaccinated.
Re:”25% incidence of infection in those w 3 doses vs 18-20% incidence in those w 4 doses at 30 days. ”
Isn’t it mainly about hospitalizations, not rates of infection?
General internist here still in practice at age 68 in Southern California. Your thoughts mirror mine exactly. Look forward to your periodic essays on ID (and life too)! I find them somehow reassuring -though not necessarily optimistic….
The other question I get asked, is, after 3 doses of Pfizeer, is it time to broaden the immune response with a Moderna dose of 50 (or even 100) mcg? Or vice-versa. I know you want an mRNA booster after J&J…
I recommend reading the article titled “mRNA-1273 and BNT162b2 COVID-19 vaccines elicit antibodies with differences in Fc-mediated effector functions” in Science Translational Medicine, published online on March 29, 2022. In terms of the breadth of coverage, the 2 vaccines seem complementary in some respects.
I am seeing Long COVID in some of my patients who have had “mild” cases of COVID. Seeing plenty of breakthrough infections now in my students, who are all required to be vaccinated and boostered. My vigilance against this tricky virus remains high. Sometimes I feel like Dr. Seuss: I do not want a mild case. I do not want an asymptomatic case. I do not want it here or there. I do not want it anywhere. I do not want it today. I do not want it tomorrow. I do not want it ever. (It maybe wishful thinking, but I’m still doing all I can to avoid becoming infected.)
Good thinking. I managed, in spite of extreme vigilence, to pick up a “mild” SARS-CoV-2 infection. It took me about a month to feel decent again.
I’ve had both vaccines and the booster.
I still wear n95 in all indoor public places. My mom’s cancer treatment rendered the COVID-19 vaccine ineffective. She has, however, had EUVSHELD.
My friends were all equally as cautious as I have been – fully vaccinated and n95s in public – and I felt comfortable visiting in their homes on occasion (3 people at the most).
A few weeks ago they all stopped masking. I’m my mother’s primary caretaker. I don’t think I can spend time with them anymore unless its outside.
I need to keep my mom safe but I don’t want to keep her locked in the house either. My sister and her family have stopped masking too…. So no weekend visits to their house anymore either.
The transition to complacency is largely the result of the widespread adoption of the flawed thinking of Dr. Robert Malone. He had saturation prime time exposure on cable news and social media. His speech on the steps of the Lincoln Memorial was covered extensively. He was featured at CPAC. In an online survey, 20% of respondents believe he is an ID expert.
I saw the unimpressive data about the 4th Pfizer shot in Israel, but at 85 my wife and I (a retired physician), decided in January during the big wave to go to a pharmacy and persuade the man to give us the fourth shot. We should probably expect to get another in September to give us a little extra protection for the winter, though by then there may be new things happening.
Please comment on dose 4. Should we mix and match.
How prevalent is long covid among those with mild cases?
Todd, what is asinine is to use repurposed drugs like Ivermectin that was *proven* in multiple studies to not work provide positive outcomes, regardless of what day it was given. Get your head out of the rabbit hole and read more reliable actual medical information, please. And the vaccine is no longer a trial vaccine- it has been well tested all over the world. While you have been isolated surfing the internet for Q-anon conspiracy, research has been adding to the knowledge base. I am surprised your post got through the moderators.
COVID is still a mysterious infection. Research has not answered many of the questions concerning this disease. I personally think that mankind would have faired much better by allowing the virus to spread through the population and burning itself out. Apparently the vaccines don’t stop infection or spread. The vaccines could possibly lead to more mutations of the virus thus perpetuating the problems. We just don’t have the answers. It seems asinine to not utilize repurposed pharmaceuticals like hydroxichloroquine and ivermectin in the fight. Instead we are given a trial vaccine that appears to have many unpredictable side effects that, in some cases, are worse than the disease itself. This virus seems to be a gain of function nightmare loose in the world. The ultimate end result of which cannot be determined. Would it not have been more prudent to let it take its course. Sure, we would have lost loved ones and many would have carried the effects of long term COVID. But in the end, it would be over. Now, those of us that chose to take the vaccine, we don’t know what’s happening inside us. Blood clots, heart attacks, strokes, and more may be coming down the proverbial road. Our nation needs to heal both body and soul.
I’m sorry, Todd, but your understanding of epidemiology may be lacking. Smallpox was never eradicated by letting it spread through the population. It spread for several hundred years until medicine came up with an effective vaccine and basically vaccinated the world. The same with polio and Diptheria, which killed millions of children. A new study just outlined the rate of heart swelling (cardiomyopathy) in those vaccinated vs non-vaccinated. Rates of all types of heart disease in the non-vaccinated following a Covid illness were very much higher than the minimal cases of cardiomyopathy from vaccines. No one vaccinated has died from a cardiomyopathy. The vaccines are NOT worse than the illness itself. It is not ok to let people die who could have been saved with the medical treatments available, just to lessen the inconvenience others experience. My husband has CLL. He has had 4 vaccines now, along with Evusheld. Without vaccines, those with even mild CLL have a very high death rate. With vaccines, it is still 1 in 3 who will die. A cavalier attitude to just letting him die from Covid is unacceptable when he is a viable functioning smart human being that I want with me for a considerably longer time. As to those in care homes, etc, it is not our choice either to just let them die when there are treatments available, unless someone has the clarity and capacity to legally refuse treatment or has given that decision-making option legally to someone else.
“Reported” cases/infections up 30 to 40 percent in Connecticut, Massachusetts, New Jersey & New Yotk. Correct me if I am wrong … is not this 5th or 6th Spike since 3/2020? Have not we seen this Horror Movie before? Apparently, those folks with Diabetes are very vulnerable to serious illness. Repeat after me this is a worldwide Pandemic that is NOT over. Bryan in Walnut Creek, CA.
You’re right about Diabetes. I know a person in his 70’s with Diabetes who was triple vaccinated and died in February. There needs to be more information about this to those who have it. He thought he was protected by the vaccines, and he took chances he didn’t need to take. There needs to be more effort put into helping people with Diabetes reverse it through healthy diet. (Yes, it’s possible, call it “remission” if it makes you feel better).
There also needs to be more effort made to prevent Type II Diabetes. It’s very hard to change the entrenched eating habits of many. A start would be to allow nutrition education throughout grade school. I’m aware of a teacher who tried that but was told to stop as a parent complained that she couldn’t afford the foods the nutrition facts recommended. One in 5 children in America are hungry and nutritionally deprived every day. Also, we need to provide basic health care for all Americans as modernized countries around the world have now, including even Russia. Take a look at all the countries who do provide it, allowing for reaching more of those who need medical care. https://en.wikipedia.org/wiki/List_of_countries_with_universal_health_care
Also important, would be to eradicate the use of High Fructose Corn Syrup which the pancreas cannot metabolize and instead converts HFCS to fatty liver and weight gain. The last administration allowed the corporations to change their labeling so now one doesn’t know if a product contains “fructose” as to what type of fructose is it – natural or artificial. This benefits the corporations monetary gain but is physically harming many Americans. Some European countries have a production quota on it’s use now.
I find te level of craven bleating in comments to be repulsive. You people are living with a highly contagious but mildly consequential variant. Get back to how the human race used to see life; there will always, and there always needs to be, risk. The world, and your lives, will never be ‘safe’ so stop whining.
I find your insinuation that infectious disease doctors are craven bleaters to be repulsive. I also find that you deciding what risks others must take so you can “live your life” selfish.
Feel free to take YOUR own risks by jumping off mountains or speed racing. Not by being nonchalant about a communicable disease with the possibility of morbidity or mortality for others.
But, I guess ID doctors and healthcare experts are whining.
Dr Balfour:
The Vermin only tease and pinch
Their Foes superior by an Inch.
So, Naturalists observe, a Flea
Hath smaller Fleas that on him prey,
And these have smaller yet to bite ’em,
And so proceed ad infinitum:
Thus every Poet, in his Kind
Is bit by him that comes behind
Peace!
Jonathan Swift
Do you have any insight as to why you’re so angry? Having a contrary opinion is one thing. (Though expecting agreement or sympathy in Dr Sax’s blog is certain to go awry.) Has something happened that was really hurtful?
You assert the phenomenon he explains- a vast denominator, much worse than even a bad influenza year. Do you sincerely believe nearly a million deaths is ‘mildly consequential”? And your invective and pejorative verbiage are indicative of real fury. Why so?
Very sensible (and I defer to your expertise). My non-expert guess is you will be proven correct to worry.
I keep wondering what’s coming with BA.2. One news source I skimmed today said public health experts do not expect another surge. I didn’t read the details.
Among the many things COVID-19 has taught us is that forecasting and prognostication in public health are more often than not a fool’s errand.
The human population and billions of organisms have evolved and learned to live with each other over millennia. This learning has come through natural infections, therapeutics as well as vaccines which saved billions of lives and sufferings. The only success story of eliminating infectious agent small pox virus, should be considered serendipity and a miracle. Polio could be nearest rival still separated by eons despite vaccines.
Covid will be no different. We must strive to save lives and sufferings by all possible means. Yes, some may get mildly infected but most will be saved.
ID or non ID physicians, we all are part of the mechanism to make it happen.
Article on mixing and matching boosters: https://www.statnews.com/2021/10/12/a-primer-on-what-we-know-about-mixing-and-matching-covid-vaccines/
An editorial by Ezekial Emanuel in today’s Washington Post seems apropos:
https://www.washingtonpost.com/opinions/2022/05/12/stop-dismissing-long-covid-pandemic-symptoms/
Dr. Emanuel summarized many of my concerns.