
An ongoing dialogue on HIV/AIDS, infectious diseases,
November 16th, 2023
Being a Good Doctor — Why Are the Simple Things So Hard?
The simple things that make someone not just a doctor — but a good doctor — can slip away from us when we’re too busy, or tired, or preoccupied, or hungry. That’s why it’s wise periodically to be reminded of the “soft skills” that, while individually not tricky, together make a huge difference in how patients perceive us.
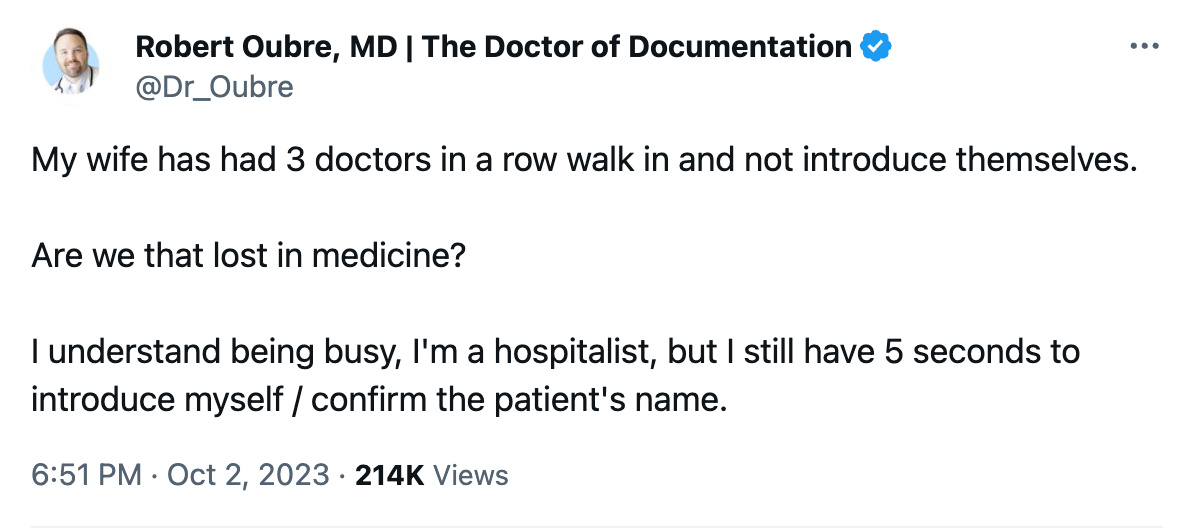
“Soft skills,” by the way, is the term coined recently by Dr. Robert Oubre, a hospitalist from Louisiana who specializes in Clinical Documentation Improvement, or CDI. Periodically imparting his wisdom on social media and in his newsletter, he recently posted something entitled, “Preventing and Protecting Against Lawsuits.” Here’s what one lawyer told him was a critical part of avoiding legal trouble during patient care:
You should practice in a way that causes your patients, and everyone you work with, to like you.
Be likable! How sensible. Because beyond lawsuit protection, I’d argue these soft skill make up critical components of patient care, and legal risk-reduction is just a corollary benefit.
Here are some of those skills he cites, in bold, followed by my comments — it’s a great list. He writes from the perspective of hospital care, but a lot of them transfer over to the clinic.
Sit. In the hospital, patients are often in bed, sometimes in a chair, but hardly ever standing. Get on their level. This small physical act greatly increases their sense that you care about them and that you’re giving them time. Logistically, it’s not always easy — family might be visiting, chairs might be occupied or have stuff on them, the room might be architecturally challenging. But try to make it happen when you can.
Call. Find out who they’ve listed as their designated family member or friend to help out, and keep that person updated. We had the importance of this action driven home to us during the dark days of the pandemic, when families couldn’t visit. One time-saving strategy is to have the patient call while you’re rounding in the room or during the office visit, and put their family member on speaker phone.
Ask, “What questions do you have?” rather than “Do you have any questions?” The former invites questions, the latter subtly discourages them.
Introduce yourself. Patients meet a ton of clinicians during their hospitalization, especially if it’s a long and complex one. Coverage changes, weekends and holidays happen, specialists aplenty get called in. For many services, the era of working extended blocks of time of consecutive days is long gone. So it never hurts to remind patients who you are — and do it repeatedly, as with rare exceptions, we are terrible with names. (You lucky few out there who are good with names are fortunate indeed!) During his wife’s recent care, Dr. Oubre posted the following — that empty, confused feeling when people fail to introduce themselves:
Use the patient’s name. There’s really no excuse for not greeting the patient by their name — after all, we all know it, it’s right at the top of the medical record. So use it — “Good morning, Mr. Smith”, “Hello again, Ms. Lopez”, “Hi, Mr. Gupta, how was your night?”, etc. (Then introduce yourself — again. See above.) If the name is unfamiliar or hard to pronounce, ask them how to pronounce it, and do your best to get it right. Plus, on those occasions when a patient changes rooms, this action provides another check that you’re not about to take a history, do a physical exam, or worst of all, do a procedure on the wrong person. (Yes, it happens.)
Acknowledge others in the room — and find out who they are. I added that last bit. Both are crucial. Let’s imagine you walk in the room, and your patient (a man) is accompanied by a woman. Try this script: “Hello Mr. White, I’m Dr. Schwartz, nice to meet you.” Turn now to the woman, and say, “And who do we have with us today?” Not — “… and is this your wife?” Most of the time it will be the spouse or partner — but not always. Everyone has made the mistake of assuming it’s a spouse, only to find out it’s the patient’s friend, or sibling, or parole officer, or daughter (ugh), or mother (ugh again). If you haven’t yet made this embarrassing generational error, learn from our mistakes and don’t do it yourself.
Corollary to this point: On rare occasions, your patient doesn’t want the extra person there, but has been forced (or even bullied) into it. Give them an opportunity to be alone with you, by asking if they’d like the person to be there during the history or during the physical exam. For young adults (ages 18-25, give or take), I typically allow the parents in the room during the initial history, then ask them to leave during the physical at which time I can ask more delicate and private questions.
American Theater Poster, 1899
Mention the NAME of other doctors that are caring for them. While you may not be able to do this for all the doctors, try at least to name the primary attending physician, or in the outpatient setting, the referring clinician. And don’t just mention their name — tell them you’ve been communicating. “I heard from Dr. Li, your primary care doctor, that you had a positive TB blood test and had some questions”, or “I know from reviewing your chart that Dr. Aslam thinks you might need a change in antibiotics.” With so many people involved in a patient’s care, it’s critical to inform them that everyone is working as a team to help them get better — “Establish a team-work mentality” is another one of Dr. Oubre’s soft skills, and this strategy affirms this team work.
Smile. Listen. Affirm their experiences. One patient I saw with severe asthma told me how grateful she felt when one of our gifted pulmonologists said something like, “That must be very scary for you” when she described the sensation of having an asthma attack. Remarkably, in all the years of seeing various clinicians, no one had ever mentioned that before. Having this doctor acknowledge her fear went a long way to establishing their very successful long-term care plan.
For our new HIV diagnoses, we make sure to acknowledge the feelings they have when they find out their HIV test returned positive — something along the lines of, “It can be hard to hear that the test is positive.” Then pause, and let them speak. We can then quickly move on to reassure them that the diagnosis is no longer a death sentence, that treatment can lead to a long and normal life, and that we’ll help them adjust to this new reality of having a chronic (but treatable!) condition.
Follow up on promises. My wonderful (and still dearly missed) late colleague Paul Farmer took this to heart more than anyone I’ve met. No matter how busy or crazy his schedule, if he told a patient he’d be back to hear more of their story, or to give them boots, he’d do it. (Here’s the boots story, #2 in the list.) I’m not saying we need to buy everyone boots — but his actions stand out as a good model for what we should aim for.
Be approachable to nurses. This statement, of course, applies to all the members of the care team. There’s no room in good patient care for outdated hierarchies or authoritarian actions. The nurses, social workers, pharmacists, front desk staff, the person delivering the food tray, transport personnel — we’re all there to accomplish the same thing, which is to get our patients better. The more we acknowledge and validate the others we work with, the better we’ll do.
Remember to look at them — not just the computer. Sure, we can consult the electronic medical record during the visit — just tell them that’s what you’re doing, and even apologize if you need to go on a lengthy search. Or invite them over to do it with you! But staring exclusively at the computer screen and typing while seeing a patient is a surefire way to create distance between “us” and “them.” And yes, I added this one to the list, as it’s long been a pet peeve of mine.
A non-medical person reading the above might think this stuff is easy. What’s the big deal? But trust me, the fact they seem so obvious stands in sharp contrast to just how difficult they are to do consistently, in particular when external demands weigh in as distractions.
But try we must — not only to avoid lawsuits (the original purpose of Dr. Oubre’s excellent list), but just to be a kind and caring doctor.
Anything left out you want to mention?
It certainly never hurts to ask about pets — people love talking about their pets, especially if they have a special talent.
27 Responses to “Being a Good Doctor — Why Are the Simple Things So Hard?”

Paul E. Sax, MD
Contributing Editor
NEJM Journal Watch
Infectious Diseases
Biography | Disclosures | Summaries
Learn more about HIV and ID Observations.
 NEJM Journal Watch — Recent Infectious Disease Articles
NEJM Journal Watch — Recent Infectious Disease Articles- Observations from ID and Beyond: Hot Takes from IDWeek: CDC, COVID, and Two Doses of Dalbavancin
- Frailty Predicts Outcomes in Resistant Klebsiella pneumoniae Bacteremia
- Should Recipients of Kidney Transplants Receive Treatment for Asymptomatic Bacteriuria?
- COVID-19 mRNA Vaccines Aid Immune Checkpoint Inhibitor Cancer Therapy
- Cefiderocol in Health Care–Associated Gram-Negative Bacteremia
Avoid sitting on the bed. If you do need to sit on the bed, put your hand down first to make sure it’s dry. It might save you from an unpleasant surprise.
A Doctor should remember to knock first before entering the room.
Yes! And take a couple of seconds to wait for a possible “Come in” or other response.
All so true and need to be built into and practiced as part of any medical school curriculum
It seems a little crazy in retrospect, but at Hopkins my patients all had my direct office number and e-mail address, and I would check my messages when I was out of town or out of the country. If I returned their calls when I was away, I would always mention where I was calling from, and it paid off! Some of my patients had never been outside of Baltimore. Even years later they would remind me that I had once returned their call all the way from New York, Los Angeles or Paris.
I agree! Patients are pleasantly surprised when I email or call them back mentioning that I on vacation in another state or country. They almost always apologize for bothering me.
I also ask whoever is with the patient if they have any questions to make sure their concerns are addressed. However after reading this article I will change it to the better version of “what questions do you have”.
I had a pulmonologist ask me “What question can I answer?” And after the first question she asked “And what other question?” And after that question, yet again until all my questions were answered. It let me know that she was not looking to get the visit over with quickly before all my questions were answered. Patients are often fearful of taking up too much of a doctor’s time.
These are all nice, thoughtful and caring things to do when caring for patients. I’d likely endorse most of them. However, whether these niceties are effective malpractice mitigation strategies remains unproven.
I think that the suggested conduct will likely get you a 4-5 star rating, but I suspect that they’ll have no measurable impact on litigation.
when I go to the bank many tellers call me Mr. William. When I answer a phone call from people who want something from me they ALWAYS,say “is this “William”? When did this
obscene practice get approval from the courtesy police?.
Sir William Osler noted that it was more important to know who the patient is than what the disease is.
I have suggested to patients and friends that they might pose this question to their doctor, making direct eye contact:
“ Do you want to know who I am?”
If the answer or vibe is unsatisfactory, another doctor may be more appropriate.
What Osler said was probably true for him.. A similar saying is that “the patient does not
care how much you know ,until he knows how much you care”.
Soft skills can be useful. Today ,however ,I believe the greater truth is that the patient “does not care how much you care until he knows how much you know.”
Always. make a physical contact, may be just a gentle handshake (Warmth of both hands is welcome) or a hand on the shoulder or a caressing gentle strokes of the hand over the forehead. Must always do a small act that you care, besides the supra, handing over the spectacles or papers in the bed side drawer, or just tidying up the shirt-pyjama or the bed.
Agree! Specially true when seeing elderly patients who live alone. I always listen to their heart and lungs even if the visit could have been done with no physical contact. It may be the only physical contact the have with another person.
This is in the book “My Country” by Abraham Vergese … the part goes: A paliative care HIV patient was admitted and even to the very end of his life, every time the doctor entered the room and talked some, this patient would unbutton his gown for the physical as if a ritual between the two … Very good book by the way
Reference asking about pets no harm to broaden out the question to : ” what do you like to do in your spare time ?”
Also a good fall back strategy if communication is faltering on either sides !!
Excellent point about the first name ! The greater the age difference (older patient with new young doctor) the more inappropriate it feels to be called by your first name . Especially if the doctor is white and patient is non white.
I agree with the comments about not addressing a person by their first name unless this has been established as the preferred way previously (such as long term outpatient relationships). I also always check to see if the person has a title other than Mr, Ms, – so being sure to call PhDs, MDs, DOs “doctor” and retired military personnel but their rank – Colonel Jones, Captain Smith and so on. That goes a long way towards showing the person you have a sense of who they are outside the role of patient.
This was a fantastic topic and the wonderful comments only added to its benefit. One of my Palliative Medicine colleagues told me years ago that sitting when in the room gave the impression that 5-10 minutes there was 20-30 minutes if the patient where asked later. This is not too be deceptive but to show you how important it is to sit. I would add that I always ask if the patient has served in the military AND where he or she was stationed during service. I did it for disease exposure sites originally but am now a history freak and always love hearing about military service stories. The patient, as you might expect, is very endeared to those asking these questions and I am always amazed at some incredible feats of valor or survival.
In my 42 years as an internist and pulmonologist, I could NEVER bring myself to call patients by their first name on an initial visit unless we knew each other socially. I might move to a first name relationship after really getting to know the person. My assistants always called patients by their last names. Recently I was summoned from my PCP’s waiting room by a very young assistant, whom I’d never met, calling me by my first name. It was most disconcerting and inappropriate.
Really well put. It can be hard to do this every day and all the time, but even getting 90% of it right 90% of the time makes a huge difference. Once a doctor is on the other side of the chasm – lying in bed as a patient – it is much easier to see all the problems with not introducing oneself or not acknowledging that life-threatening illnesses are scary and humbling.
Most of my patients have my mobile number. There was an advertising campaign for an Australian bank a few years ago all about, “do you have your bank manager’s mobile?” It struck me as odd that I did have my bank manager’s mobile, but my patients didn’t have mine, for arguably even more important and urgent conversations. It has very rarely been abused, but has been life-saving at least once – a patient was about to hop onto a long-haul flight but just wanted to ask about his severe breathlessness and whether it was ok before he departed. The massive pulmonary embolism was successfully thrombolysed and he did well.
Long live HIV and ID Observations!
All my patients have access to me with text messaging me through our EMR. Many of my patients also have my cell phone number. I give it out liberally to patients and their family, specially when a patient has a new serious diagnosis or is entering hospice. I agree that this is rarely abused.
Male patient/female doctor, female patient/male doctor. Some unusual situations may cause embarassment!
I have been in the same, large primary care practice for 28 years. I have know most of my patients for many years (some 28 years). One of the best ways to develop good patient/provider relationships is to stay put.
After I have introduced myself I acknowledge ever one in the room.
This lifts the heavy air from the room 90 % of the time.
I tell patients that when I walk into the room I am among family. Then I quip ” good or bad” you are still family.
A careful and respectful touch goes a long way in building rapport.
After sensing patients’ religeous leanings I invoke God and his will.
I donot have any concrete data but I feel letting the patient sense a caring environment can certainly avoid most unpleasant situation.
I am a hospitalist and carry a three-legged cane with me at all times so I always have a place to sit by the patient’s bedside. It takes awhile to get used to carrying it around with you in the hospital but once you get used to it, it is invaluable.
I also always give my business card with my cell phone on the back and let patients know the nurses can get hold of me but to call me if they need to. Also to tell any family members who need explanations to feel free to call me directly. It saves a lot of time and will often help catch errors that I would not have known about until much later. One of the biggest frustrations that I hear from friends who have had family in the hospital is that they cannot get hold of the doctor.
This article hits the nail on the head! It’s often the simplest aspects of being a doctor that prove to be the most challenging. From active listening to showing empathy, these foundational elements can sometimes get lost in the shuffle of medical training and the demands of a busy healthcare environment. Yet, they’re absolutely essential for building trust with patients and delivering truly patient-centered care. It’s a reminder to all of us in the medical profession to continuously prioritize and hone these skills, as they are what truly make a good doctor great. https://asprius.in/