
An ongoing dialogue on HIV/AIDS, infectious diseases,
September 13th, 2020
Restaurants Are Hurting — But Dining Indoors Poses Real COVID-19 Risk
As we learn more about transmission of SARS-CoV-2, the news for restaurants goes from bad to worse.
And while there’s a long list of sad things about this pandemic, the decimation of the restaurant business for owners and the people who work there is right up there. The loss of the restaurant experience for us diners is pretty sad, too.
Importantly, restaurant dining isn’t one of those hypothetical risks for COVID-19, such as surface contamination of groceries and delivered packages. It’s a real, well-documented concern with strong supporting evidence.
In a CDC study conducted at 11 healthcare facilities and just published last week, investigators queried 154 people with symptoms consistent with COVID-19 and positive tests, along with 160 control individuals testing negative. They asked about various activities in the two weeks prior to the onset of symptoms — eating out, shopping, going to an office, visiting a hair salon, taking public transportation, attending a religious service, and others.
People with positive test results were more than twice as likely to have reported dining at a restaurant than were those who tested negative. No other activity conferred significant risk.
It’s a small study, and the authors note several potential limitations, but they amplify the message that crowded settings, close contact, and lack of mask wearing indoors increase the risk of COVID-19.
The vagaries of restaurant ventilation — so exquisitely detailed in this investigation of a restaurant outbreak in China — add to the hazards of indoor dining.
Here, one presymptomatic person infected nine other diners, all of whom sat under the the same air conditioning vent that recirculated “old” rather than fresh air.
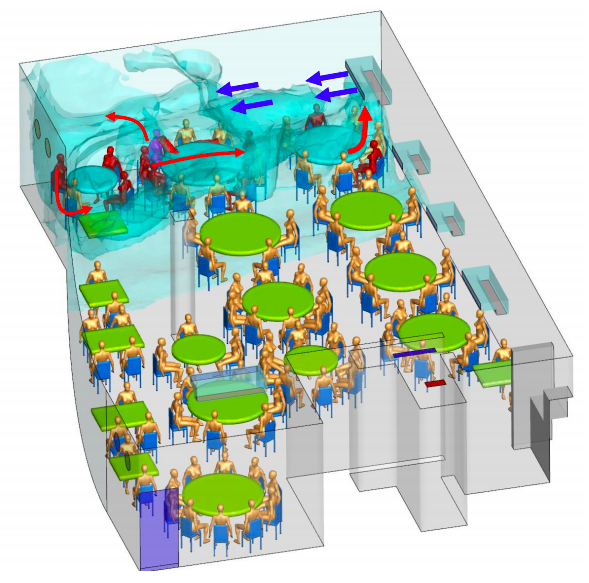
www.medrxiv.org/content/10.1101/2020.04.16.20067728v1.full.pdf
None of the 68 diners in other areas developed COVID-19, nor did any of the 8 waiters — likely because transient contact is much lower risk.
Meanwhile, Harvard epidemiologist Professor Miguel Hernan compares epidemic curves in New York and Madrid in this fascinating thread:
1/
Look at the shape of these curves.New York and Madrid had similar epidemics until they spectacularly diverged.
In March, both cities were caught by surprise and shut down because of #COVID19.
In September, the situation is under control in NY and alarming in Madrid.
Why? pic.twitter.com/VF0BCl0xyt
— Miguel Hernán (@_MiguelHernan) September 11, 2020
What does this have to do with restaurants?
In New York, indoor dining is CLOSED. Indoor dining in Madrid was OPEN at 60% capacity in June. Bar service opened too. Protocols weren’t aggressively enforced. Since June it has been easy to find crowded bars and tables. The contrast with NY was striking as anyone spending time in both places can tell you.
Is it too far fetched to extrapolate from these cross-city comparisons and conclude that opening restaurants played a role? Not really, when you consider how cases in the southern US spiked when bars and restaurants opened in regions that still had significant community transmission.
(And having had the pleasure of dining late — and I mean late — into the evening in Madrid, I can assure you that these meals are the very opposite of transient when it comes to potential exposure time.)
As noted above, all this information about restaurants and COVID-19 risk makes me very sad. Having grown up in New York — arguably one of the world’s great restaurant cities — I love the way a top restaurant experience provides more than just excellent food. The atmosphere, the conversational buzz, the decor, the rituals, and of course the intermingling of so many different cultures enhance our lives in countless ways. Certainly I’m not alone in missing this colorful aspect of life from the Before Times.
Not only that, but my mother worked as a food writer, and for years wrote a weekly column in the New York Daily News on hidden restaurant gems in the city. If a new Ecuadorian restaurant opened in Queens that generated some buzz, you can be sure we’d soon be sampling some empanadas ecuatorianas or llapingachos.
Meanwhile, awaiting a vaccine and other preventive strategies, what can we do now to support these hurting restaurants?
Dine outside while we can. Tip heavily. Order take out. Buy merchandise. Other ideas here.
But skip the indoor dining in restaurants for now. And while we miss it, it might help to remember that eating out isn’t always so great.
https://youtu.be/K_q4S7lZeik
27 Responses to “Restaurants Are Hurting — But Dining Indoors Poses Real COVID-19 Risk”

Paul E. Sax, MD
Contributing Editor
NEJM Journal Watch
Infectious Diseases
Biography | Disclosures | Summaries
Learn more about HIV and ID Observations.
I heard that some pubs in villages in England immediately started home delivery including a beer with a main meal. Could we do that here please. We have been isolating since the last week of February..and would love a pub meal or similar, but not enough “to die for”. Maybe if there hadn’t bee the job keep, maybe then we would have had some home deliveries? sigh.
Also with summer coming up, obviously outdoor dining is the way to go, suitably spaced up to maybe 15 in a group around a few tables, separated from other groups of tables by at least three metres if possible, so one can walk between them and not be too close!.
It is interesting to see the development of the New York / Madrid curves. In my opinion there could be an alternative explanation to that of the restaurants and that is that NY has not implemented, since mid-March, an aggressive policy of deprivation of rights of citizens and it was left more in the hands of individual responsibility to carry out or not the preventive conducts of SARS-Cov2 transmission, this entailed a substantial herd immunity (not only as a serological prevalence, but also of a cell type not routinely detectable).
Is it like that?
Perhaps it “just petered out by itself” in NYC?
Perhaps lung-cancer causes cigarette smoking.
Perhaps many things.
https://share.icloud.com/photos/0622-M4IPOsRejFRNlvxczRdw
There’s little evidence of enough herd immunity in New York to account for this difference. Only a few neighborhoods in NY experienced enough infection to have developed even close to herd immunity.
Um, no. Herd immunity requires somewhere around 70% of the population to have been exposed to the virus and develop antibodies. Even considering there are a lot of asymptomatic cases, we are nowhere near that level of exposure. Studies of the rate of people carrying the antibodies were still way below a 10% when people began receiving the vaccine. The idea of “herd immunity” through many, many people being infected quickly is a pipe dream that would lead to about 7 million deaths in the U.S. alone. The way to herd immunity is through vaccination. Done right, millions of people can be vaccinated quickly with a minuscule number exhibiting side effects more significant than mild soreness and fever. If we get to a 70% vaccination level we can be pretty sure the other 30% will be spread thinly enough in the population that outbreaks will quickly die out.
Why haven’t techniques been employed to mitigate the indoor concentration of virus in restaurants. There are ventilation systems that are employed in medical facilities which clear other pathogens like Tuberculosis. These use UV energy to inactivate the pathogen. These methods involve applying the UV energy in the ceiling area of the room away from the occupants, or having the energy applied to the air as it circulates through the ventilation system. There exists home UV air purifier units which come in two sizes and suggest that they are able to clear 300sq ft to 600sq ft. If it can be demonstrated that these type of units can clear the air contaminated as illustrated in the picture in your article, would this make indoor spaces safer? Multiple units could be deployed depending on the size of the room or larger units could be designed. Just a thought.
Also the use of outdoor heating units like the ones that are used in ski resorts might be useful to extend the outdoor dining season.
I have been interested in the use of so-called upper room germicidal UVC since the pandemic started. There is a “Viewpoint” article in the July 14th, 2020 issue of JAMA by Dr. Edward Nardell from Brigham and woman’s Hospital addressing the issue n(“Airborne Spread of SARS-CoV-2 and a Potential Role for Air Disinfection”). I have a personal concern for my grandchildren in school settings, so in investigating the history of the use of this technology dating back to the 1930’s, I was interested to read of Wells’s use of this technology to mitigate a measles epidemic in two Pennsylvania schools in the 1940’s. Unfortunatley, his work was not replicated for a variety of reasons, but the technology is used in healthcare settings, particularly in facilities dealing with TB. Retrofitting existing HVAC systems with upper room germicidal UV equipment is relatively inexpensive, compared to completely replacing HVAC systems. I believe this should be investigated further and implemented widely in high-risk indoor spaces such as restaurants and classrooms, as well as other “high-risk” spaces.
Dr. Ellis,
Do you have any idea what kind of margin the typical resturaunt operates on?
As a restaurant vet—the require “ppe” like ventilation infrastructure is 1) very expensive for a struggling operation and 2) often times may involve other city/state agencies related to buildings and fire code. (Ie: reinventing HVAC in a pre war residential building) And there is currently very little guidance on this level that is evidence based and preventative. so most operators don’t even know about filtering air like a hospital—just a few notes from the inside.
Why is it exactly that restaurants are such a high-risk environment for developing severe COVID-19? I think the reason is clear – dining close to someone with active infection ensures a large viral inoculum – a critical point that seems to have been ignored until recently (perhaps because it is not easy to study in a randomized trial).
NEJM recently published an article that highlights the issue of inoculum size. “Facial Masking for Covid-19 — Potential for “Variolation” as We Await a Vaccine” in the September 8th issue was a very important article which probably failed to get the attention it deserved because of its unfortunate title and the fact that masking has become a highly politicized issue. However, for me it suggests a new approach toward dealing with the pandemic.
Since much of the spread of COVID-19 is being driven by young people who are much less likely to develop severe symptoms to begin with, an approach of strict universal masking WITHOUT social distancing in fully open schools and universities is much more likely to create the numbers of asymptomatic and minimally symptomatic cases needed to reach herd immunity.
Even sports games and concerts could continue normally for low-risk attendees as long as masking is universal and strictly enforced (concessions would not be able to be brought into the event). Two meter social distancing would still be needed among older people, and those at high risk due to obesity or illness. “Low density areas” in stadiums and concert halls could be reserved for those at high risk.
Under such an approach, venues in which strict universal masking without social distancing is not possible such as restaurants, bars, and school cafeterias would likely need to be closed.
Dr. Adi J. Neuman
Internal Medicine
When recently I also read the article by N.Eng.J. Regarding the possible “vaccine effect” of the masks, what came to mind is that they avoid the “annual immune training” due to exposure to the different catarrhal viruses. So even the most clumsy viruses will be overwhelmed this coming fall / winter.
???
If there is a country that has taken the use of the mask to the extreme, it has been Spain. However, judging by the evolution curve it has not been very useful, nor has it been a “vaccine effect”. Dr. Roger Kimber, like you, also supported the natural development of herd immunity, shielding the population at risk for severe COVID-19 and it certainly seems like a reasonable option. The problem is that if we assume 5-10% of hospital admissions, there would not be enough beds. We have the rapid vaccination of the population. In this sense, the detractors will say that there has not been enough time for trials and it could be true with the new RNA / DNA vaccines, but if we have experience with the recombinant HbsAg of hepatitis B and we already have recombinant protein S from SARS- CoV 2. There is no need for unexpected adverse effects (https://share.icloud.com/photos/0622-M4IPOsRejFRNlvxczRdw. https://www.nature.com/articles/d41586-020-01221-y
Dr. Arturo Azpiroz,
From my family practice, we have tested ~75 +/- patients; based on clinical symptoms and/or contact. Today, my nurse and I by recollection guessed at 10+ positives, 2 hospitalized, one middle aged man briefly and one high risk individual for several days and still on bipap. Assuming 5-10% false negative tests, our population had something over 13-16 identified/identifiable cases for a hospitalization rate of 12.5-18 % over roughly 5 months. There is an unknown number of sub clinical cases (asymptomatic + not sick enough to seek care) out there that probably out number the symptomatic cases by anywhere from 3-20 times, I would guess. And, if we use the knowledge of who is likely to get sick & reverse quarantine or semi reverse quarantine them and judiciously use Ivermectin, Hcq+Zn+Az in high risk outpatients as a recent AmJ of Med article suggested (along with the Henry Ford Hospital system’s experience suggests be done; quarantine college students on campus (they are really not going to behave–think of the endemicity of STDs in this setting, get real), maybe even fill the stadiums up with loudly cheering students, they would probably all have been exposed and recovered by mid-terms and immune to go home for Thanksgiving safely with Grandma & Grandpa. If that works out, you could expand to employees under 30, etc, etc.
People are getting quarantine fatigue, others are committing suicide, others are killing other people (how much of the riots are in part fueled by COVID madness?), deaths from ODs and DWIs (both perp & victim), people who have or will die because they are too afraid of catching COVID to go to the hospital for their MI or stroke–at a time where we actually have effective treatment for these things. And that is just mortality, not morbidity! In all due deference to Dr. Sax and his ID expertise, the collatoral damage is going to be, if not already greater than that of COVID. However, no one is going document this (though we have plenty of direct and indirect evidence for each thing I have cited. Time to turn this ship around!
Finally, if the bar for approval of a vaccine is 50% effective & using historical numbers on voluntary vaccine uptake in the general population (25-33% is probably generous) doing the math you are talking about somewhere between 12.5–16.5 (50% effective) to generously 16.5–21.8% (assuming 66% vaccine effectiveness) of the population become immune from the vaccine, (absent CCP levels of coercion, which will not be tolerated). Vaccine makes good political theater & money for the manufacturers and academics writing grants, etc.
The real bang for the buck is having the COVID equivalent of Chickenpox parties that those of us of a certain age did for our children when there was a case of chicken pox in town–as older you are when you get the inevitable case, the sicker you are–kinda like COVID-19. See my comment about locking students on college campuses until they are all immune.
Dr. Roger Kimber
I can’t help but nod and admire the firmness and direction of his words. In my opinion, in Spain, we possibly had a “window period” after the first wave of COVID-19 during which something similar could have been done. At the present time nursing homes have become involved again and it is no longer possible to separate people at risk of severe infection from the “healthy” population. Apart from the virus, what proliferates are unfounded prohibitions, misinformation and fear of the undocumented.
Do not take my words as anything other than personal opinion. Regards
Thank you for your kind and generous words, Dr. Azpiroz.
In 1969, as a high school senior, I spent 10 days in Spain (Holy Week) on a trip organized for virtually all the Spanish students in our high school by our Spanish teacher, a refugee from Castro’s Cuba, and a wonderful teacher–I get complements all the time from my Spanish speaking patients on my accent–not so much my grammar or vocabulary. Whirlwind tour Madrid & environs, Toledo, Cordoba, Sevilla, Granada, Malaga. It was wonderful and a blur. Several passion play parades as I recall. I courted my now wife there(She was a better Spanish student, and our teacher played match maker. Fond memories. I will have to dust off my pictures!
Regards to you as well.
“Why is it exactly that restaurants are such a high-risk environment for developing severe COVID-19?”
I think the importance of the transmission event is underestimated. Both the site of exposure and the dose are crucial. Airborne transmission is particularly toxic as virus heads direct to lungs. Non-inhaled transmission lodging in mouth or nose might be safer. Not much research here but macaques got milder disease from conjunctival transmission compared to intra-tracheal.
I like very much your point if view.
I am a retired physician, age 80. I have a few concomitant conditions (high blood pressure, mild asthma, and diabetes Type II, all under good control). As with other communities and other people of our age, we have been confined inside our house for the past several months. Several times my wife and I feel that we must break this, get out, and eat restaurant food. We have, so far, resisted our impulse of eating restaurant food for a few reasons. The primary one is our high-risk status. Secondly, we do not know (nor can we know) if the restaurant workers use sanitary techniques for cooking. In the interest of safety and our own health, we have consistently resisted going out and eating restaurant food. Please consider the advantages of staying home: You could possibly try newer recipes, spend quality time with your wife/partner, and try to understand your loved one better. I recommend the same to our friends in similar age groups and high-risk categories. This will keep us all in a good healthy stage and lessen the burden on the community by being sick.
The study is interesting but the write-up could be better. When the author writes that it is “twice as likely” that a ‘positive’ individual dined in as that a ‘negative’ one did, it could be either relative risk or odds ratio that is reported; the word ‘likely’ suggests the former, but the author could make this absolutely clear (and reporting the complete two-way table would permit the reader to calculate either.) The number who were infected is not given for either group, so that calculation cannot be made. It is also worth noting that this is a retrospective, case-control study in which the probability, or ‘risk’ of getting sick cannot be estimated from the data. Only odds for getting sick can be estimated. Therefore only the odds ratio, not the relative risk, would be a valid statistic for the data. Given a known prevalence – and ignoring that actual disease status is replaced by a screening test result here -, Bayes’ Rule could be used to estimate Pr(Sick | dining in restaurant ), although confounding variables abound. For instance, is dining in positively correlated with going to church, to a ftf classroom, to meeting inside with others than those in one’s own household, to going to rallies or sports events if possible where one lives, to not wearing a face mask, to traveling?
One might ask why restaurants have not grouped to acquire large, unused venues such as defunct big-box establishment. They could then set up seating with tables ten or twelve feet apart from each other, with waitpersons from several restaurants available. Meals could be transported in heated containers from the base restaurants. Any municipality with a closed down Sams, Builders Square, Office Max, etc. would be a candidate for such a collaborative venture, with appropriate changes in decor, including restrooms. The typical Mall dining pavillion with several restaurant (typically fast-food) options is a prototype for the larger concept of a Pandemic Mixed Eatery.
Excellent idea!
Ambiance?
Who wants to go to Walmart or Home Depot for a romantic anniversary dinner, or to propose?
Please read the Chinese restaurant study. The index patient was not presymptomatic. He was hospitalized “later that day” after eating lunch. Has it never occurred to anyone that patients lie to tracers, especially in China?? Note in the CDC “study” that the authors cite 5 serious limitations to their study. which question its validity: journalists seem to ignore these.
I have followed your advice and have read the article. It seems that the data does not quite fit. Three tables are described: A is in the center and is where the index patient (A1) sits, in the area furthest from the air conditioner, next to table B, which is the most distant. Table C is “under” the air conditioning, next to three future patients from table A. Theoretically, the table that receives the greatest contagious impact from A1 is table B (they are very close and the air is blowing in their favor), however the first to get sick are those at table C. This seems to go against the viral load density … etc.
Will the emergence of a new contagion depend on exposure to more than one SARS-Cov2 carrier in a short period of time?
It is evident that people who go to restaurants have a more intense social life than those who do not and there would be more opportunity to be exposed to a virus processed at different stages by different hosts.
??? https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6784293/ https://www.pnas.org/content/106/14/5871
Kudos to you Paul for tagging the exquisite “Fawlty Towers” dining experience!