
An ongoing dialogue on HIV/AIDS, infectious diseases,
September 7th, 2013
FAX machines, and the Special Power of the MD Degree
Everyone hates mindless paperwork.
But certain types are particularly annoying, seemingly designed to send you screaming into the night, dragging a broken fax machine behind you as your brain explodes.
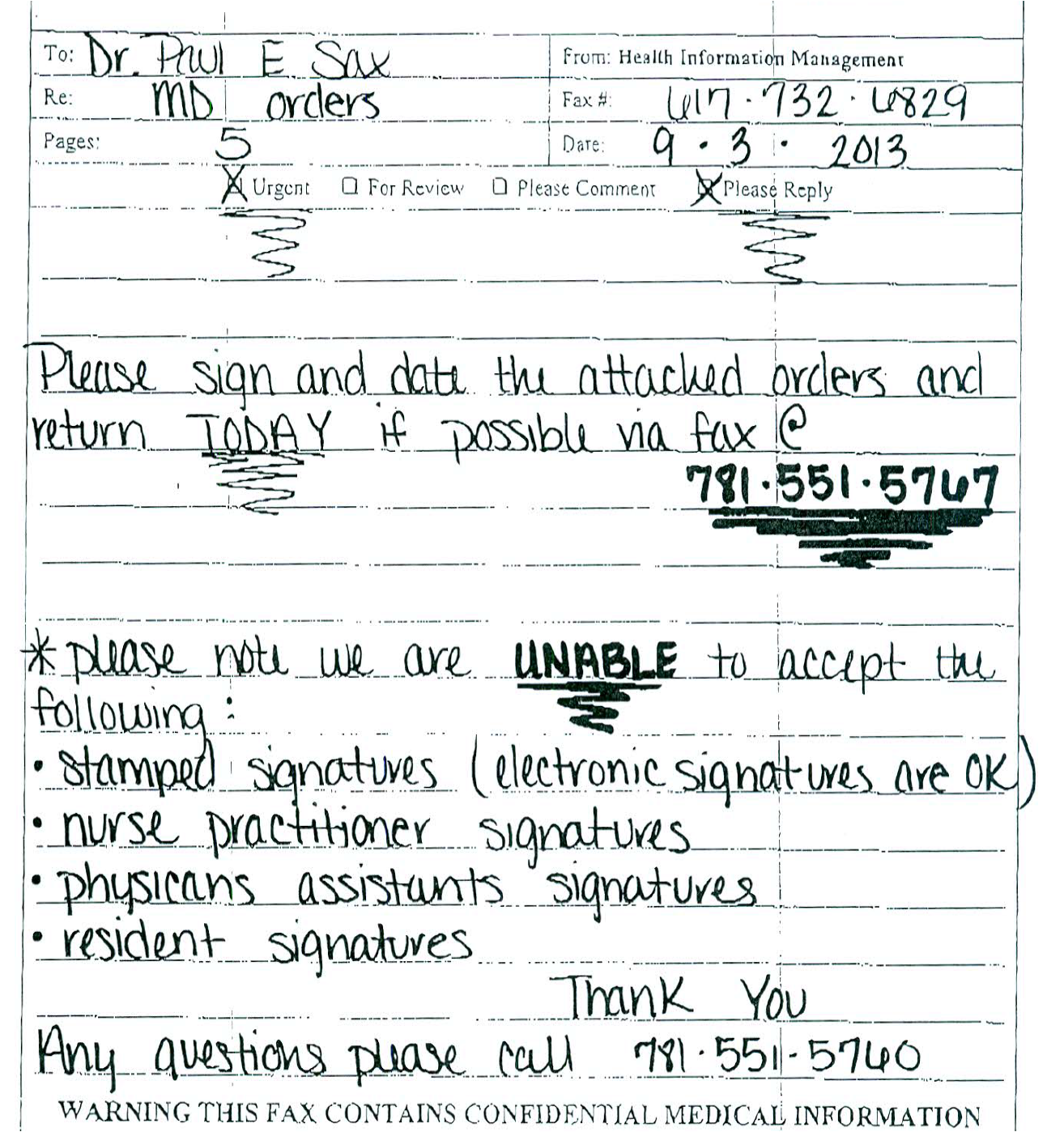
Too strong? Take a look at this fax cover sheet I recently received about a patient who had been receiving IV antibiotics at home:
To get at the root of why this particular communication rankles so, let’s do a close reading of the cover sheet — an explication, a detailed description of the prosody and narrative arc, to borrow some words from my English-major days.
Starting at the top, working down:
- It’s from “Health Information Management”: Even though names have changed a lot over the years — hardly anyone was named “Sophia” or “Emma” back when I was a kid — it’s highly unlikely that “Health Information Management” is the name of the person who sent this handwritten note.
- It’s 5 pages. Pages 1 is this cover sheet. Pages 2, 3, and 4 are boilerplate documentation of what has already been done. And page #5 is a task that raises paperwork to a new level of torture — it asks for my signature in 4 ways: 1) Slow signature; 2) Fast signature; 3) Initials; 4) Printed name. That’s a first for me, let’s hope it’s the last.
- It’s “Urgent.” Not just Urgent, but urgent!!! How do we know? Look, the word has squiggly underlining — that means it must be really important. But one might wonder why it’s so important when, as mentioned above, the care has already been given (and, for the record, the patient no longer needs their services, he’s much improved). Could it be that that the definition of “urgent” for this company differs quite substantially from a clinician’s? To a clinician, examples of “urgent” problems include a patient who is short of breath, or bleeding, or having chest pain. For this company, “urgent” means “we want to be paid as soon as possible.”
- They want it “TODAY.” See above, for “urgent”, though now they’ve brought out the all-caps, along with the same squiggly underlining. Clearly, they want me to stop whatever I’m doing and sign the form — 4 times — NOW. One company admitted they stamp all their forms “SECOND REQUEST!!!” — even first requests — as they found this made doctors respond more rapidly to their queries. Sneaky.
- This is all happening by fax. The fax machine is a virtually obsolete form of communication, soon to take its place besides dial phones, signal flags, and smoke signals. But not for home care companies — they love fax machines. They love them so much that the fax number doesn’t just have the squiggly underlining, it also is BOLDED. I can just imagine the office where Health Information Management sits — wall-to-wall fax machines, each carefully monitored, and each shrill fax tone a thrilling announcement that a doctor’s signed (4 times) order is incoming. What joy. (Small aside about fax machines: Over the telephone, “Sax” sounds just like “fax” — which meant back in the heyday of fax machines in the 1990s, I received plenty of correspondence — even faxes — to a “Dr. Fax.”)
- They are unable to accept certain signatures. No stamps. No signatures from NPs or PAs. Nothing from residents. In case it’s not clear, they’ve done something very special with the word “unable” — the triple-whammy of ALL-CAPS, BOLD, and of course our friend the squiggly underline. Must be very important. But think about this for a moment: Can’t residents write orders in the hospital? Prescribe medications to their outpatients? Do various procedures? And PAs and NPs do routine office visits, plus more complex tasks such as covering inpatient medical and surgical services, even performing colonoscopies. So residents, PAs and NPs can do these things — and do them well — but they can’t sign these forms? Maybe the PA and NP curricula don’t include the special class we MDs took on how to sign our name 4 different ways (slow, fast, initials, and print). And that special class isn’t given to just any MD — just those who are board-certified, credentialed, and have completed their post-graduate training. I’d go so far as to say that our ability to sign these forms (4 times) is the true meaning of working to the highest level of our esteemed MD degrees.
OK, I’ll stop now.
7 Responses to “FAX machines, and the Special Power of the MD Degree”

Paul E. Sax, MD
Contributing Editor
NEJM Journal Watch
Infectious Diseases
Biography | Disclosures | Summaries
Learn more about HIV and ID Observations.
 NEJM Journal Watch — Recent Infectious Disease Articles
NEJM Journal Watch — Recent Infectious Disease Articles- Botulism Cases in Babies Have Been Linked to Infant Formula
- What's the Effect of Delayed Surgery for Septic Arthritis?
- Community-Acquired Meningitis: Watch Out for Klebsiella
- Observations from ID and Beyond: Hot Takes from IDWeek: CDC, COVID, and Two Doses of Dalbavancin
- Frailty Predicts Outcomes in Resistant Klebsiella pneumoniae Bacteremia
Paul,
I cannot tell you how often this happens..But I am capable of doing all the work but do not the capability to sign my work…infuriating for NPs and I am sure PAs as well.
But the time lost to assist patients for timely paperwork is delayed as well .
Thankyou for pointing this out and your acknowledgement for the work we do recognized and affirmed…
Meg,
The rules about signatures on these things are very bizarre, almost arbitrary. I can only guess what’s behind them. Maybe (just maybe?) it has something to do with money — payors make it deliberately difficult to get documentation that the care was ordered, which helps them delay payments. The homecare companies pass this off to us. Or maybe I’m being too cynical …
Paul
Paul,
As a mostly-primary-care doctor who does some HIV care, I can’t tell you how many of these I sign. My HIV+ patients are a tiny portion of this story; but the rest of my panel is a constant fire hydrant of this stuff. (So much that it not uncommonly takes them saying “Third Request! Extremely Urgent!” to get me going.)
To me this is part of something larger, which I simultaneously understand and resent.
Understand: These homecare orders represent billions (with a “b”) of taxpayer dollars. The government has to ask, who is going to certify that this is a legitimate expense? Is it someone who is paid by a hospital (that’s the NP, PA, or resident), which might have a financial relationship with the home healthcare agency, and who can ultimately be ordered or coerced to sign based on the dictates of their employer? The agency themselves, or the patient, either of which is an obvious way to make billions into trillions?–want a scooter with that home PT? Or is it the person with ultimate responsibility for the care, who not incidentally has the most to lose from committing Medicare fraud, and who should generally not have a financial relationship with the home health agency? On a policy level, I think this is part of the reason the answer should be the doctor, and not just any doctor, but the attending.
Additionally, the more annoying you make the process, the more that doctors will only order it if they think it’s actually needed. Again, NPs, PAs, and even residents can be made to do annoying things all day if economic interests demand it; attendings are a harder sell.
As a primary care doctor, these signatures for home health, diabetes supplies, wheelchairs, and disability applications represent me personally, just me, actually moving potentially hundreds of thousands of dollars in tax money in as short a time as a week, certainly in a month. (And I am a minor player compared to docs who have much more geriatric panels, who might be moving hundreds of thousands of dollars in a busy day.)
If not the ultimately responsible physician, who else should decide such an economically and clinically important set of decisions?
And yet I resent here what I also resent in medical marijuana. In some ways, we are being asked to be arbiters of our society’s ambivalences. Society wants to take care of sick people but doesn’t want to pay for it. Society doesn’t think marijuana is that big a deal but also isn’t ready to pay for it. Who do we get to solve this problem? If we get a doctor’s signature, it will mean that this thing we are ambivalent about is actually OK.
The irony is that the more we require this “enforcement” mechanism the more that you get to the point where doctors are just going to sign whatever piece of paper comes in front of them as long as it has some familiar-sounding patient’s name on it.
In a rational system I personally think we would just let people smoke marijuana or not let them, and stop asking doctors to make that OK.
And in a rational system we would decide that care in the community is the responsibility of an integrated system of care (i.e., your clinic’s nurse goes out to the patient’s houses, not some random agency nominated by a rehab case manager on discharge day); or, alternatively, that care in the community is simply not a public responsibility.
What makes me saddest about it? Signing these orders is just one part of the medical-industrial process I need to keep up with which makes it nearly impossible for me to go to my patient’s homes.
Joe
Often it is the state licensing laws that prevent providers other than MD/DO’s from signing documentation. I deal with this complication regularly in my own practice, having to ask a colleague to sign off on care I ordered, for my own patient. No chance that I would be coerced to request unneeded care, just an outdated law that can’t conceptualize other categories of licensed independent providers.
The answer to this one is Medicare Part B reimbursement. NP’s and PA’s are reimbursed at 85% of MD’s for Part B (home health, durable medical equipment). When the visit/procedure is billed with an MD as the ordering provider under which the NP/PA is practicing, reimbursement is full. Here’s the official CMS document on this, which is called “incident to” billing.
“A nonphysician practitioner such as a physician assistant or a nurse practitioner may be licensed under State law to perform a specific medical procedure and may be able (see Section 190 or 200, respectively) to perform the procedure without physician supervision and have the service separately covered and paid for by Medicare as a physician assistant’s or nurse practitioner’s service. However, in order to have that same service covered as incident to the services of a physician, it must be performed under the direct supervision of the physician as an integral part of the physician’s personal in-office service. As explained in Section 60.1, this does not mean that each occasion of an incidental service performed by a nonphysician practitioner must always be the occasion of a service actually rendered by the physician. It does mean that there must have been a direct, personal, professional service furnished by the physician to initiate the course of treatment of which the service being performed by the nonphysician practitioner is an incidental part, and there must be subsequent services by the physician of a frequency that reflects his or her continuing active participation in and management of the course of treatment.”
Of course, no one is checking your active participation. They are looking for your valuable signature, taking final responsibility for what mid-level providers ordered.
Disclaimer: Everything I’ve said here is knowledge gleaned over the years from asking different people and googling, not any formal training – kind of like how I practice medicine. (I kid, fellow NP’s)
Dr. Sax,
I agree with everything you’re saying… but the tactics of using underlyining and saying this is the second notice, those are just strategies they’ve used to get doctor’s to respond faster. From their perspective, I can kind of understand these tactics, even though drives me crazy as a physician.
What I cannot, for the life of me, understand is why they still insist on using fax machines!!! It is so inefficient and takes up a sizeable portion of a department secretary’s day just dealing with routing faxes, getting them signed, and faxing them back. We should start charging them a fee or something to communicate through faxes. It’s just ridiculous.
Paul, thx for this! It made me laugh, it made me cry…