
May 19th, 2020
Safety Net: Reflections on the Elmhurst Experience
Eric Bressman, MD
Dr. Bressman is a Chief Resident in Internal Medicine at Icahn School of Medicine at Mount Sinai in New York, NY
Elmhurst 2014
I first arrived at Elmhurst Hospital in Queens, NY, in the summer of 2014 as a medical student on my surgery rotation. We would take occasional night shifts as part of the trauma team. It was the first time I held a pager. Code yellow meant hurry, code red meant run. One of our first patients was a code red, a young man, not much older than I am now, who had fallen several stories from a rooftop.
I remember a few things from that night: the humid July air; the symphonic chaos of the operating room; running through the halls of the hospital, from the OR to the blood bank and back, as the impromptu courier for the massive transfusion protocol. What remains most vividly in my mind, however, is standing outside his bay in the SICU, after he had briefly been stabilized, and hearing his father thank us, through tears, for doing everything we could. His prognosis was grim, but his family remained appreciative, nonetheless.
 I have returned to Elmhurst every year since then, for weeks or months at a time, first as a medical student, then as an intern, a resident, and a chief resident. Although only a few miles away, it has always been a world apart from hospital life in Manhattan. The hierarchies less rigid, the class lines less visible, the rhythm entirely its own. And in a city where the patients can be exacting, at Elmhurst they have been, on the whole, gracious and grateful for the care they receive, even under difficult circumstances.
I have returned to Elmhurst every year since then, for weeks or months at a time, first as a medical student, then as an intern, a resident, and a chief resident. Although only a few miles away, it has always been a world apart from hospital life in Manhattan. The hierarchies less rigid, the class lines less visible, the rhythm entirely its own. And in a city where the patients can be exacting, at Elmhurst they have been, on the whole, gracious and grateful for the care they receive, even under difficult circumstances.
Elmhurst 2020
When we first heard about a novel pathogen wreaking havoc on major cities and beginning its inexorable march around the world, our thoughts turned to Elmhurst. The demographics of the neighborhood and the relative paucity of healthcare infrastructure servicing the community all pointed toward a perfect storm. It is easily one of the most diverse square miles in the world; about 70% of the population is foreign-born. Every direction you walk from the hospital finds you immersed in a different outpost of transplanted culture and distant national pride. Its proximity to two major airports makes it the point of first contact for many new arrivals to the U.S. who require healthcare. On a normal day, Elmhurst sees disease processes that are relatively common in the developing world, but generally buried in the footnotes of U.S. medical textbooks.
When it came to SARS-COV-2, the neighborhood was not so much a melting pot as a pressure cooker. For a host of reasons — including tighter living quarters and holding essential jobs that did not afford the luxury of working from home — social distancing was not a simple option for much of this community. Within a couple of weeks of the first confirmed case in New York, Elmhurst was overrun with COVID-19. This was a code red.
The latter half of March was a complete blur. Regular wards turned into ICUs overnight. Multiple codes an hour. An incomprehensible daily death count. Overflowing morgues and freezer trucks outside the building. Patients came in, got intubated, and died so quickly that often there was no time to obtain a family contact. They died alone, while their loved ones waited by the phone.
Elmhurst’s Future
There will be time to count the losses, to recount what took place here. There will be stories of personal sacrifice, of staff stretched to the limit, of fear and fearlessness, of the trauma of uncertainty. There will be a necessary examination of what was missing and how we can better prepare for the next wave or the next pathogen. But we must be careful, too, because anyone who has spent any time around Elmhurst, or similar safety net hospitals, knows this: There are no heroes and there are no villains. There are only dedicated but overburdened staff, working tirelessly with limited resources, and victims — of an indiscriminate virus, and a broken system.
There is a nagging, painful question I can’t quite get out of my head: If these patients had shown up somewhere else — if they had crossed the East River and found a hospital with more ICU beds and more critical care staff — might some of them have been saved? But this misses the point entirely. The question we should be asking is why Queens, a borough the size of Houston, has fewer than 200 ICU beds. Why a population larger than that in neighboring Manhattan is serviced by threefold fewer acute care beds, primarily at public hospitals and community affiliates of larger academic medical centers based across the river. The battle here was over before it started. There was no amount of curve-flattening that could bring the peak within range of capacity.
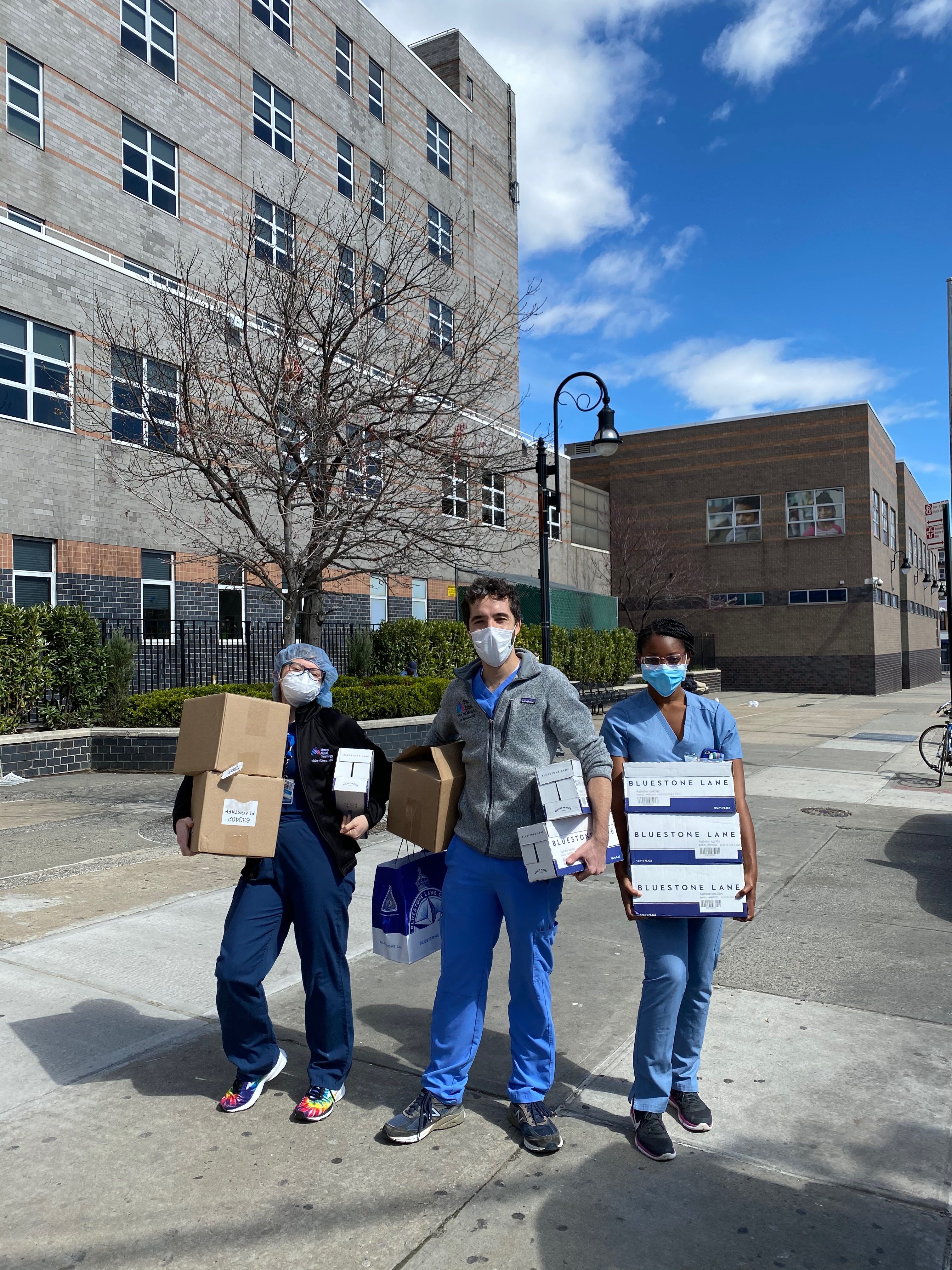
Elmhurst has been stabilized. And the community, through tears, is thanking us, showering us with food and gifts and words of encouragement. The staff deserves it. But our city, our system, does not deserve their gratitude. We deserve an outpouring of anger and demands for more resources. This can be a moment of unity while still being an impetus for change.
Safety nets are there to catch us when we fall, but they can only bear so much burden. A system designed to chase a certain payer mix will, over time, leave communities with high proportions of the under- and uninsured overly reliant on underfunded public hospitals. Universal health coverage is an imperative step, but we also need a more cohesive system that can allocate resources thoughtfully and equitably, rather than by the guiding principles of the invisible hand. Elmhurst will carry on, even as it fades from the public view. This moment, however, will be defined not only by what we did, but by how we responded to it.

6 Responses to “Safety Net: Reflections on the Elmhurst Experience”

2021-2022 Chief Resident Panel
Abdullah Al-abcha, MD
Mikita Arora, MD
Madiha Khan, DO
Khalid A. Shalaby, MBBCh
Brandon Temte, DO
Resident chiefs in hospital, internal, and family medicine
Learn more about Insights on Residency Training.
 NEJM Journal Watch – Recent General Medicine Articles
NEJM Journal Watch – Recent General Medicine Articles- Haloperidol: Time to Retire QT-Prolongation Hypervigilance?
- Shingles Vaccination Probably Protects Against Heart Disease
- Should Hospitalized Patients Receive Normal Saline or Lactated Ringer's Solution?
- Is ABG Necessary to Diagnose Hypercarbic Respiratory Failure?
- West Nile Virus Infection: Get Ready for an Uptick in Cases
Brilliant piece. I work at an FQHC. Business currently dominates medicine, shapes the scope of services and targeted population even in nonprofits like mine. We need an equitable solution and emphasis on key services. Thank you for sharing your experience
I read and re-read your essay through tears of grief, astonishment and anger. You are so very correct in your assessment and eloquent in your words.
Thank you for writing this powerful and thoughtful reflection! As a fellow Chief Resident at a safety-net community hospital, I could not agree more that we need an equitable healthcare system that cares for its more vulnerable.
Cheers,
Frances
This was such a powerful piece!
Thank you for sharing. More power to all of you
Excellent commentary. I have been and continue to be a patient requiring the services at Elmhurst Hospital for almost ten years now. I agree with your synopsis of the unfortunate and dire situation at my hospital. Of concern is that it may have stabilized for the moment only. I fear what I see is the inevitable return of chaos and loss.
I am a Foreign-born, US educated with a high degree of education, long-term resident of Elmhurst neighborhood heaconsumer/occasional patient. One major problem of this facility is mentioned by the author himself stating that “gracious and gratitude” pervades from patients despite hardships. Well, should you “the discontented” or the over-worked doctors, nurses, support staff then assume the leadership in challenging the status quo of your institutions to make equitable health care to those neighborhood past the Ed Koch aka 59th street bridge? Or would you or perhaps the union-protected staff remain just comfortable with the way it has stabilized? These 70% foreign-born Elmhurst residents are not as sophisticated or aggressive as those in zip codes like 10021 in demanding exact compliance to the standards of care. We need help. We have many stacks going against us including equitable housing, employment and now made visible by covid 19, health care. As a retired clinical man, I ask people like you or your colleagues, to please remember the interconnectedness of health care, housing and labor in having a just society. We have very limited voice, failing to keep nearby St. John’s hospital to remain open, a few years ago. We are the disinfranchized second-class residents. Tired with fighting abusive landlords, employers, we ask help as much as possible. Thank you.