
February 26th, 2020
Medicare for All: The Healthcare Our Nation Needs
Frances Ue, MD, MPH

Dr. Ue is a Chief Resident in Internal Medicine at Cambridge Health Alliance in MA.
Over a month into the new year and feels like the world around us is in grave peril. There are many reasons to lose hope: the climate crisis with Australia’s wildfires, the evolving COVID-19 epidemic, the acquittal of the President’s impeachment charges, and the list goes on. Combined with long hours, sick patients, and seemingly never-ending grey skies in Boston, it can feel challenging to find goodness in the world.
In search of inspiration, I often turn to my colleagues at Cambridge Health Alliance. One such colleague is Dr. Adam Gaffney, a critical care doctor, public health researcher, activist, and president of Physicians for a National Health Program (PNHP). I had the pleasure of interviewing him for this blog.
(Interview transcript edited for length)
Me: Tell us about yourself. How did you become involved in activist work?
 Adam: Well I’ve been pretty progressive politically for my whole adult life but, during residency, I began to be more active in PNHP. It was a time when concern for inequality was rising, the aftermath of the great recession, occupy Wall Street, really a growing sense in the country that more and more people were being left behind and also clear that health care was a big part of that. I was fortunate enough to be able to join an organization that was on the front lines of speaking about the need for universal healthcare reform, and I’ve been involved in that organization ever since.
Adam: Well I’ve been pretty progressive politically for my whole adult life but, during residency, I began to be more active in PNHP. It was a time when concern for inequality was rising, the aftermath of the great recession, occupy Wall Street, really a growing sense in the country that more and more people were being left behind and also clear that health care was a big part of that. I was fortunate enough to be able to join an organization that was on the front lines of speaking about the need for universal healthcare reform, and I’ve been involved in that organization ever since.
Me: In terms of feeling passionate about Medicare for All and PNHP, can you tell us a little bit about how you discovered this as your passion?
Adam: The idea that healthcare should be a right, and should be a social good, and not a commodity, is an idea that I’ve believed in for as long as I’ve seriously thought about politics and how society should be structured. I think over the course of my medical training, I realized that this was an area where, fairly or unfairly, as a physician, I could have a much larger impact. I also had personal experiences in the course of medical training, that reinforced to me how essential it was to have a system that provided healthcare to everyone by their needs, not by their economic means.
Me: What are the key arguments for Medicare for All and how would it work practically?

Adam: Medicare for All would be a different way of paying for healthcare in this country. Right now, we pay for healthcare in a few different ways. A lot of healthcare is still paid through the government, more than half and that’s because we pay into taxes for things like Medicare for the elderly and Medicaid for low-income people. We also spend a lot of money on public employee healthcare benefits, and there is also the Veteran Affairs (VA), Department of Defense, and other federal, state, and local healthcare programs. Although we spend a lot of money on healthcare through the government, we also spend a lot through the private sector. Private insurance, co-pays, deductibles, out-of-pocket payments, also constitute a large amount of healthcare spending in the United States.
We have this fragmented, multi-payer, partially privatized way of paying for healthcare and the price is that we’ve left:
- 30 million people uninsured
- 44 million people (probably more) underinsured, meaning they have insurance but it doesn’t actually cover the costs of their care
- we’ve generated a profound amount of waste in the form of healthcare bureaucracy.
- We spend more than 800 billion dollars a year on healthcare administration like billing, which is about one third of total healthcare spending
Medicare for All would simplify the way we pay for healthcare rather than putting our money into these various different pools. All the money would flow through a single-payer (the federal government) and hospitals, doctors, drug companies, and everyone else, would be paid for by that single payer. Everyone will be covered with full universal coverage similar to other high-income nations. And because of that, everyone will have an equal level of access to the system. Finally, the way the bills are written and the way the PNHP proposal is structured, it would also eliminate out-of-pocket payments, like co-pays and deductibles. That sounds probably the most radical for many people but the truth is, that is how it works in Canada and the United Kingdom for the most part — you go to the doctor, you get hospitalized, you don’t have to pay out-of-pocket. It can be done, and it can be done affordably.
Me: How were you able to create momentum to create change as a leader and community organizer?
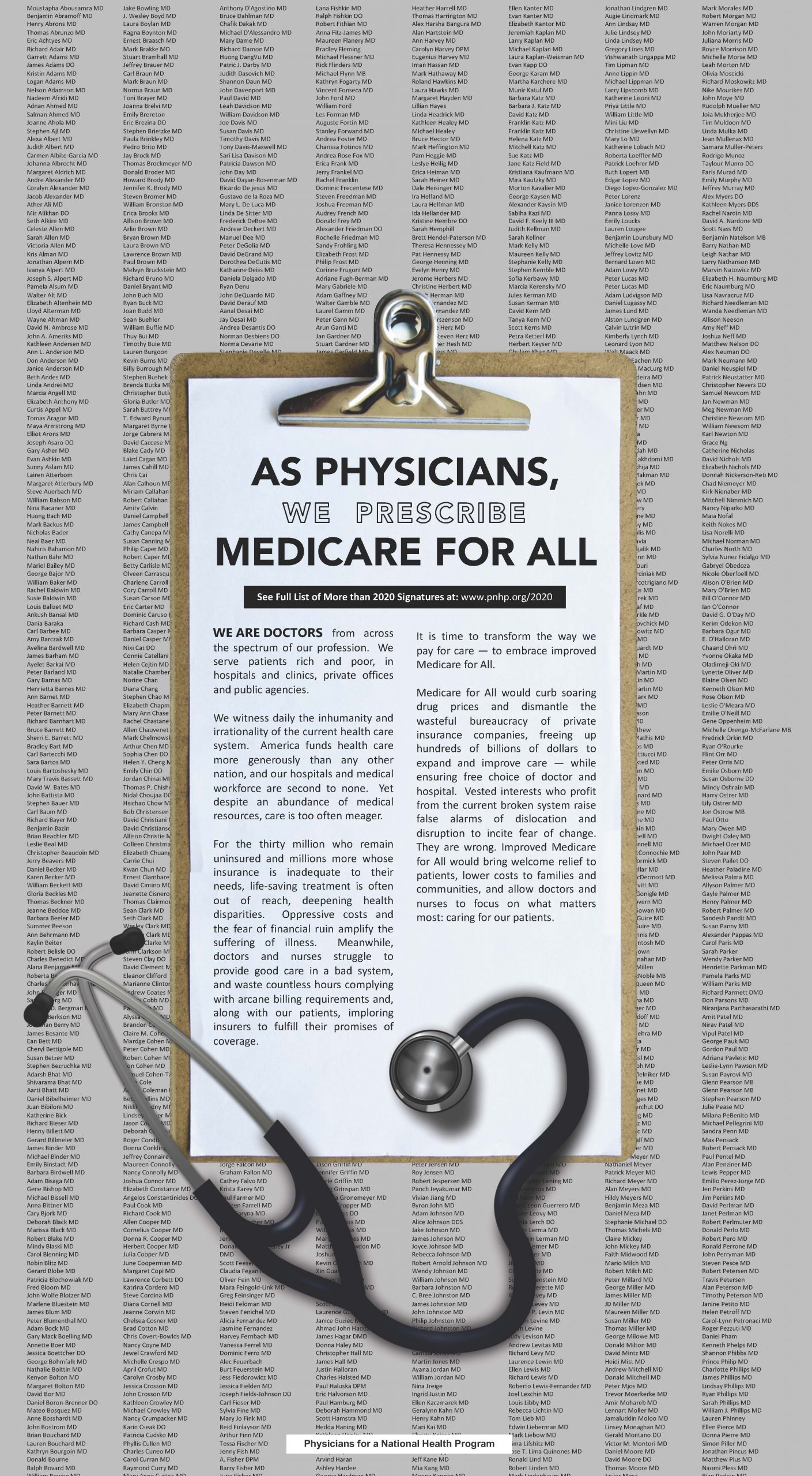
“As Physicians, We Prescribe Medicare for All”: An open-letter — signed by more than 2000 physicians — was published as a full-page ad in the New York Times on January 21, 2020.
Adam: There have been physicians and many others who have been working on this cause for decades. PNHP, for instance, was formed in the late 1980s, and members of the organization have been pushing this agenda ever since. It’s really been in the last 5 years however, that Medicare for All has swung into the mainstream discussion. And there are different reasons for that. I think that on the one hand, we had the Affordable Care Act, which helped a lot of people, but it became clear that it didn’t do enough. On the other hand, we’ve had a rise in popular, progressive politicians like Bernie Sanders in the Democratic primaries. And I think certainly, we’ve had a rise in unhappiness with the amount of inequality in our society.
I think the other reason why we’ve had some success is that it’s becoming increasingly clear that this system is not working well for physicians. And what do I mean by that? Well, physicians are having to spend more and more of their week glued to their computers, doing bureaucratic and clerical billing tasks; things that are really taking them away from the patient’s bedside. At the same time, they and hospitals, are having to hire literal armies of billers and clerical staff to do all these interactions with insurance companies (to get the payments made, to fight for the prior authorizations). It’s really not just draining emotionally and psychologically for doctors, it’s obviously taking a huge amount of resources.
We’ve had success with PNHP helping educate the medical profession about why Medicare for All reform would be very good for our patients, but also pretty good for us, too. And we’ve seen that there has been a change in the medical profession. In January, the American College of Physicians, second largest medical specialty society in the United States, came out in support of universal healthcare and explicitly endorsed Medicare for All. We also published a full-page advertisement in the New York Times, with an open letter, with the signatures of more than 2000 physicians ‘prescribing’ Medicare for All for the nation with some of the most prominent doctors in America, like Dr. Bernard Lown, the developer of the defibrillator, and Dr. Paul Farmer, founder of Partners in Health.
We’ve helped to give voice to a large number of physicians, by some polls, the majority of physicians, who do in fact support single-payer.
Me: Let’s transition from Medicare for All. How did you get involved in research and how have you used research for advocacy?
Adam: I came to Boston 8 years ago for my Pulmonary and Critical care fellowship at Massachusetts General, Brigham and Women’s, and Beth Israel hospitals. And as part of a fellowship, there is a research component. As someone interested in society and inequalities, but also in a pulmonary program, my initial research interests were actually more in respiratory epidemiology; inequalities in lung function. At that point, I also was very interested in health policy and health politics and began to realize that it may be difficult to have these very different sorts of passions. I ended up transitioning into focusing on health services research and I came to Cambridge Health Alliance, in part, because that was the kind of research I wanted to do. We have a group of people here who have long been doing this sort of research and also have long been involved in PNHP.
Since then, I’ve had an opportunity to do some studies that have examined both the ways in which the US healthcare system is not working, which are quite honestly not difficult to find and also to study how a healthcare reform might function. In three studies we did last year, we looked at, after a country moves towards universal coverage, how does it affect the society-wide utilization of healthcare services? How does that impact how many hospitalizations, how many doctor visits are used by society? And we were interested in that because that’s a big question in terms of the cost of reform.
This past January in Health Affairs, we looked at how having VA health coverage affects people going without needed medicines because of cost as opposed to other kinds of coverage. Under the VA system, copays are either very low or zero for medicines, depending on what category you fall into. And for people with other insurances, co-pays and deductibles for medicines can be hundreds or even thousands of dollars a year. So not surprisingly, we found that people with VA coverage didn’t go without needed medications because their costs are much less than those with other kinds of insurance. And it was particularly beneficial for people with low incomes and in racial and ethnic minorities.
Those are a few examples of the kind of work we’re doing which I think is really critical to achieving change. You need high-quality research, you need the numbers, you need the figures, you need to really understand the issues in order to be able to speak up both honestly and intelligently about the problems.
Me: How did you identify mentors and sponsors to help you along your way?

PNHP conference 2019 with David Bor, Danny McCormick, Adam Gaffney, Steffie Woolhandler, Janine Petito, Natalie Shure, Andy Hyatt, and David Himmelstein (L-R).
Adam: I think I was very fortunate to meet people who had shared beliefs and shared commitments. Some of my mentors, like Drs. David Himmelstein, Steffie Woolhandler, and Danny McCormick are people who I met in the course of my work through PNHP, but it turns out that they also did all these other sorts of things that I became involved with as well. I think finding people with a shared vision and shared commitments is a great way to find mentors. And they also should be people you enjoy spending time with as well, which really makes it all much easier.
Me: What’s next in your career?
Adam: The reality is, despite this being in many ways an optimistic moment in those who advocate for Medicare for All, this is going to be a long road. There is an enormous amount of work that still needs to be done for us to have universal healthcare (how will it run, how will it work?) So I think my life and my career is going to revolve around continuing to work on national health insurance and developing the knowledge base and tools, and the research that we need to make it happen. I, and many others, plan on committing ourselves to this as a lifelong pursuit.
Me: With all this experience, what advice would you give trainees who are also hoping to incorporate advocacy work into their careers?
Adam: I think it certainly can be done, but to be honest, it’s not easy as a physician because you’re pulled in many different directions. You have home and work responsibilities. Being a physician is a more than full-time job. The advice I typically give is, throughout your medical career, from medical school onwards, there’s going to be times you have opportunities to engage, there’s going to be other times when say, in the middle of your intern year, you may not be able to. And that’s okay. What you really need to do is not be harsh on yourself when you’re not able to take part in the kinds of things you want to. Just remember, you’ll have an opportunity to get back into it down the road. I think being involved in advocacy does require some sacrifices; you can’t do everything. You have to make some choices about what matters the most to you. But I think that if it’s something you’re really passionate about, you should be able to find a niche, find a position that allows you to do advocacy work. The more that it intersects with your practice or with the people you’re working with, or with your research, the more relevant it will be.
Clinical training is extremely challenging intellectually, but also, personally, and emotionally.
There are issues that we are passionate about and finding the one that speaks to you can actually help you overcome the challenges of training and of being a physician.
Thank you, Adam Gaffney, for kickstarting a series of articles profiling physician leaders, activists, and change-makers; people making a difference in the world of medicine and beyond. Learn more about PNHP and Dr. Adam Gaffney.
I welcome any suggestions for future guests! Leave a comment below or send me a tweet, Frances Ue.
21 Responses to “Medicare for All: The Healthcare Our Nation Needs”

2021-2022 Chief Resident Panel
Abdullah Al-abcha, MD
Mikita Arora, MD
Madiha Khan, DO
Khalid A. Shalaby, MBBCh
Brandon Temte, DO
Resident chiefs in hospital, internal, and family medicine
Learn more about Insights on Residency Training.
 NEJM Journal Watch – Recent General Medicine Articles
NEJM Journal Watch – Recent General Medicine Articles- Can Anyone Build an AI Chatbot That Spreads Health Disinformation?
- As-Needed Albuterol/Budesonide for Mild Asthma
- Observations from ID and Beyond: The Mystery of the Isolated Hepatitis B Core Antibody, Solved
- Initial Management of Carpal Tunnel Syndrome
- More Evidence for Ocular Adverse Events with GLP-1–Receptor Agonists
This opinion piece is rife with misinformation and partisan politics from the start. Attributing Australia’s wildfires to climate change when it was acts of arson is disingenuous at best. Then the comment about the impeachment of a duly elected president on purely party lines with zero evidence is a sad state to see educated people support.
On to the subject at hand, while it sounds wonderful in theory, in practice in the US it is neither affordable nor is the government EVER more efficient than the private sector. As a government contractor in a previous career, I have seen first hand the waste and abuse, not to mention the same politicians you so despise will now have complete control over medical making decisions for the populace. You’re advocating for no choice for anyone except the elite who can use their money to truly buy superior healthcare.
Create efficiency in the system first then expand it, not the other way around. Also be prepared to make the hard decisions like age limits for dialysis. Ostensibly, solve problems don’t create them.
The biggest inefficiencies in the system – particularly enormous administrative healthcare spending (>800 billion / annually according to a recent analysis in the Annals of Internal Medicine) and drug prices that are twice as much as what other rich countries pay – are the effect of our privatized and fragmented healthcare financing system. Creating efficiencies requires transforming the financing system.
williamhgreen@yahoo.com It sounds from here like the goal justifies the means to achieve it. Government sponsored healthcare is already very expensive, and I’m not sure that goes beyond the HHS budget for it, an idea mentioned in the article.
Healthcare as a right? Not sure how that translates into results even in the US.
Administrative efficiencies and lower drug prices can produce the savings needed for the expansion of coverage. 4 trillion dollars a year of healthcare spending is enough for a universal system without financial barriers.
Sad that young people would buy into a system that will solidify centralized control over our lives and the lives of our patients. Anyone with the slightest education knowse that it must ultimately end up as Ezekiel Emmanuel’s “Complete Lives System”, https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(09)60137-9/fulltext
It is very disheartening to see a young person advocate for a system that ultimately looks at people as a collective instead of an individual, as a ‘quality of life years adjusted’ instead of a human being. Very very immoral. What this really exposes is the immorality of our educational system which teaches our children that treating people as a collective instead of individuals is somehow moral. Why are we not treating principles of freedom and individualism to solve problems instead of then malignancy of collectivism? The NEJM should be ashamed of themselves for pushing such an unethical theology. I fear for the future for my children and grandchildren who will be subjected to the massive immorality and dehumanizing effects of socialism. TEACH FREEDOM NOT BONDAGE. Very very sad.
It is amazing that people who think we cannot afford to pay for doctors, hospitals, and medication somehow think that we can afford to pay for doctors, hospitals, medication and a government bureaucracy to administer it. Thomas Sowell
Socialism in general has a record of failure so blatant that only an intellectual could ignore or evade it.”
-Thomas Sowell
I applaud you for your efforts. Am in complete agreement that we have a failed healthcare system. It’s wasteful and full of fraud and abuse.
• Roughly a quarter of the $3.8 trillion spent on healthcare in the U.S. is wasted each year according to a study (JAMA. Published online October 7, 2019).
• We don’t need Medicare or Medicaid. Ex. hospital clinics charging facility fees. Medicare wellness visits…. We need a new system run by a separate non-profit that the politicians cannot manipulate via their craving for lobbyist monies.
• US physician practices spend more than $15.4 billion annually to report quality measures (Health Aff (Millwood). 2016;35(3):401-406).
• Many suggest that the current proposals for Medicare for All’ Is Really ‘Medicaid for All’.
There is a great deal of wasted spending. I would also point you towards this recent analysis looking at administrative spending in the US healthcare — twice as high as Canada as a proportion of total health spending.
https://annals.org/aim/article-abstract/2758511/health-care-administrative-costs-united-states-canada-2017
However, to achieve those savings we indeed need a Canadian-style single-payer financing system.
what government program isn’t fraught with fraud waste and abuse….you think Medicare for all will make that better??? The government is the cause not the solution.
Pure and simple BS: this whole generation have been brainwashed, they are beyond redemption.
unfortunately, that appears to be true…..let’s hope enough of them understand freedom that there is still hope…..progressivism is far more destructive than the corona virus…
Thank you for this discussion. I am curious as to the breakdown of financials and your estimate what Medicare for all will cost compared to the current fragmented inefficient system we currently have. I am in support of this 100%. What about private insurance?
Thank you for your comment. There have been a number of recent analyses of costs under single-payer; here are some recent ones.
Systematic review of 22 Medicare for All economic analyses found that 19/22 estimated savings:
https://journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.1003013
Recent economic analysis in Lancet looked both at economic effects and lives saved:
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(19)33019-3/fulltext
Analysis of potential administrative savings:
https://annals.org/aim/article-abstract/2758511/health-care-administrative-costs-united-states-canada-2017
Leaving a partisan comment regarding the result of the impeachment proceedings in your introductory paragraph was unfortunate. Universal Health Care will need to involve both Republicans and Democrats, liberals and conservatives if it is to be realized in the United States. Alienating those who don’t share your political view will continue to cause a divide that does not need to be present. Otherwise, an excellent discussion and interview.
Dear William,
Thanks for reading and leaving a constructive comment. The introductory paragraph is meant to reflect my own personal opinion and certainly not intended to alienate others. I agree that health care is a human right and involves everyone regardless of political affiliation.
Cheers,
Frances
Frances: health care is NOT a human right……no one is entitled to your labor as a physician…NO ONE!..That is a progressive e lie…..if you truly believed that healthcare is a ‘human right’, you would be fighting with all your might to get the incompetent, corrupt and inept government out of healthcare not increasing their role….condemning people to”The Complete Lives System’ reducing them to ‘quality of life years adjusted’ is NOT a human right. You are exhibiting immorality to even suggest so….
57 Ainslie St N,Cambridge Ont.Fully 37% of your Provincial taxes pay for the Universal Health care. Think that will fly in the US which already has a trillion in debt. There is also a difference from Province to Province as to what is covered. Ontario Canada is the economic engine of the country. Everyone is already bitching about no health care for autistic kids. Out of Province health care is either insured or paid directly by the patient. So be careful of that which you wish for. Bernie has a good idea but the taxes will not carry the day if the voter understands what Swedes pay and what other countries pay. There is “no free lunch”. Be well. PMM
Dear All, if I could discuss the Universal Healthcare concept with you I would say do not think of it as socialism, it is the exception to the rule. Britain has never been a socialist country and neither will we. We just both have socialist programs that happen to work for our needs.
Although born and raised in Wash DC I was lucky enough to live in England from 1966 to 2003 and personally experienced a National Health System with a family of 3 children. If only I could have brought the NHS home with me – it would have been the best gift ever.
We have a system with extremely high costs due to its gross mismanagement with real detriment to the user. It CANNOT put the patient first because it IS A BUSINESS! The American College of Physicians has recently endorsed a National Health System as they state it would allow them to give their patients better care. Does that not convince us?
It is indisputable that we spend 2 x the cost per person on healthcare that the UK spends for their citizens and yet we are still 34th in world ranking. If it’s broken – FIX IT!
And, a Private Health Ins for those who want that (on top of their NHS contribution) will not conflict with a National Health System. Just as it did not in the UK.
My thanks for your attention.
I find this as wishful thinking…..Do YOU and YOURs want to wait over a year for a hip replacement. Do You want to deal with NO crash cart if patient is over 70,how about NO Dialysis if you are over 55 and NO CABG if you smoke or are over 55. What about those who want Private insurance- will that be allowed. Remember Canadians can now come to the US for healthcare but not if we go single payer. Do You want to be told once you have worked hard all your life that at a certain age you no longer contribute and therefore are no longer worthy of “extra care.” Do You want the “efficient and humanistic” government to determine your health care? As for me- ABSOLUTELY NOT~!
Just to clarify, the UK does have private health insurance. Approx 10% of the citizens have this. It is also an accepted fact that the National Health System hospitals are as good if not better than the private ones.
A family member has had 2 hip replacements in the last 3 years and had an excellent recovery at 90 years old. This was a normal service available to anyone regardless of age. The other services/ treatments mentioned are also fully available.
I can confirm the astute British population would never accept “ being put out to pasture” in their latter years.
One aspect I particularly liked about the System was its simplicity – no paperwork and no bills- really!
It is not, as often said free, but it costs their country half as much per person as our Healthcare costs. I believe there will have to be some well thought out process for the US to implement a similar program but if kept simple it will work very well. And we will wonder why we did not do it sooner!
How does this optimistic young physician hope to overcome the reality of natural human law?? How can she justify the inevitable institution of Emmanuel’s “Complete Lives System”? What are we teaching our kids??
“Enactment of Medicare and Medicaid provided a direct subsidy for medical care. The cost grew much more rapidly than originally estimated—as the cost of any handout invariably does. Legislation cannot repeal the nonlegislated law of demand and supply: the lower the price, the greater the quantity demanded; at a zero price, the quantity demanded becomes infinite. Some method of rationing must be substituted for price, which invariably means administrative rationing”. M. Friedman.