
March 29th, 2017
Deep Brain Stimulation Targeting in Neurosurgery, Part II of III
Bianca Belcher, MPH, PA-C

Bianca Belcher, MPH, PA-C, practices neurosurgery in Boston, MA.
This is Part II of a three-part series on deep brain stimulation (DBS) targeting designed for providers who lack an intimate level of knowledge and/or experience with this subject matter. In Part I, the ventralis intermedius (VIM) target as well as an overview of DBS, equipment, and programming were discussed.
Globus Pallidus Internus (GPi)
Where is it located?
The GPi is located in the basal ganglia inferior and medial to both the putamen and globus pallidus externa (GPe) and just superior to the optic tract.
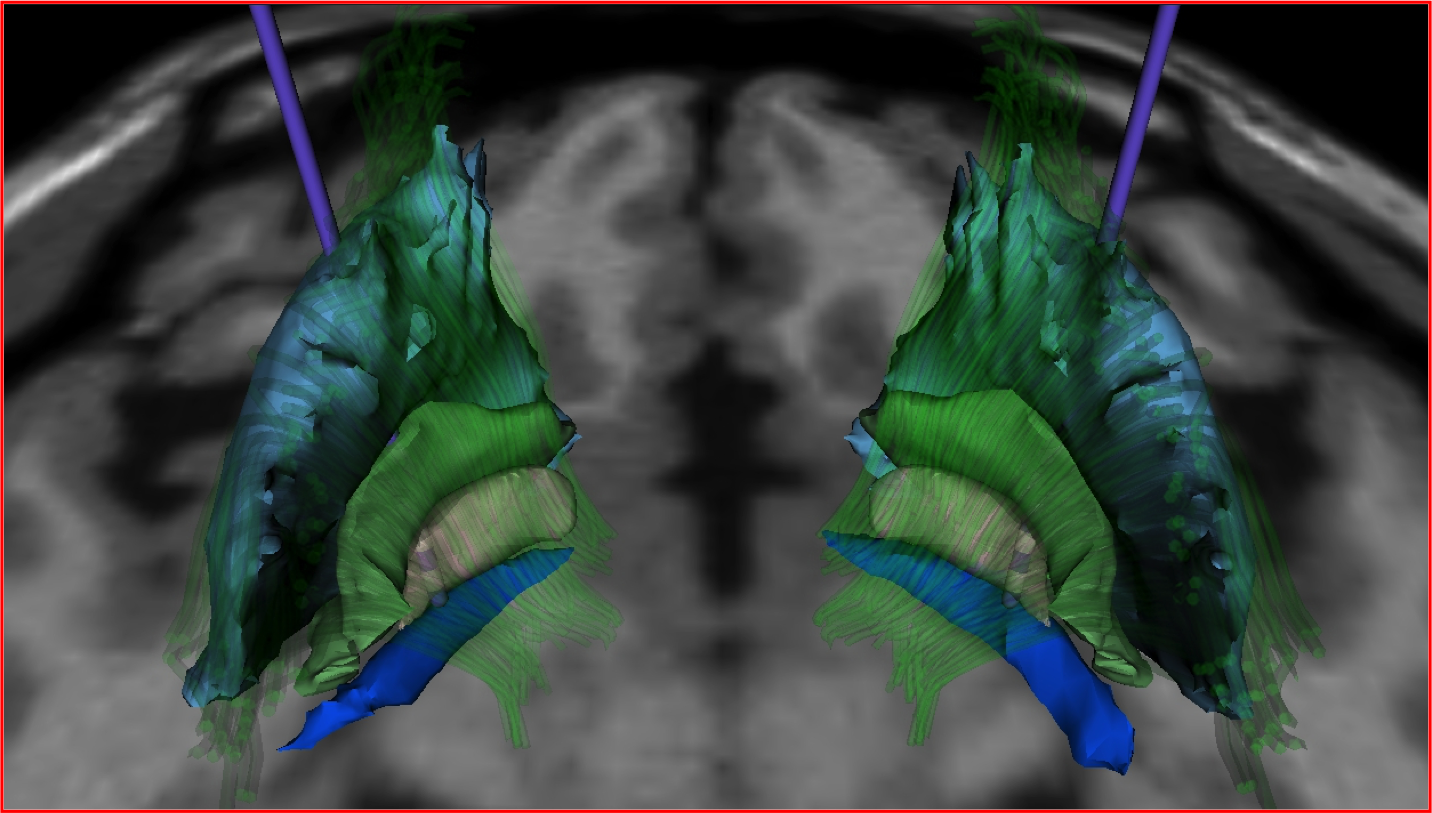
Gray, GPi. Green, GPe. Royal blue, optic tract.
Indication for Targeting:
- Parkinson’s Disease (PD)
- Stimulation of the GPi treats the cardinal motor symptoms of PD, but less effectively compared with STN stimulation.
- GPi should be considered if a patient is having significant difficulty with levodopa-induced dyskinesia but an increased dose for cognitive benefits is desired. Of note, GPi stimulation typically does not lead to a reduction in PD medication [1].
- GPi treats dystonia secondary to PD well.
- Primary dystonia
- GPi is the primary target for hereditary dystonia and generally has excellent outcomes with good patient selection.
- VIM and STN are not generally used for dystonia.
Cautions:
- GPi is a large target requiring higher voltage settings to achieve symptom improvement. This requires more frequent battery changes or the consideration of a rechargeable battery. With a young-onset PD patient, this is an important consideration over the lifetime of the patient for both cost and wear and tear on the surgical site.
- Postural instability is not well treated with GPi stimulation.

Adverse side effects of stimulation based on location of electrode in relation to optimal placement [2]:
Too lateral – With simulation of the GPe, expect to see little to no effect on symptoms.
Too medial – With stimulation of the internal capsule (located medial and posterior to the GPi), unwanted muscle contractions can occur.
Too posterior – Same effects as placement too medially
Too anterior – Little to no effect on symptoms
Too superior – Same effects as placement too laterally
Too deep – Since the optic tract lies just deep to the GPi, stimulating it results in the patient seeing phosphenes (rings or spots of light perceived by the patient without actual light entering the eye).
In Part III of this series, I will address the final most commonly used DBS target, the sub thalamic nucleus (STN).
References
- Groiss SJ, Wojtecki L, Südmeyer M, Schnitzler A. Deep Brain Stimulation in Parkinson’s Disease. Therapeutic Advances in Neurological Disorders. 2009;2(6):20-28. doi:10.1177/1756285609339382.
- DBS Anatomy & Side Effects. A Presentation by Kirk Finnis, PhD. Medtronic.


NP/PA Bloggers
Elizabeth Donahue, RN, MSN, NP‑C
Alexandra Godfrey, BSc PT, MS PA‑C
Emily F. Moore, RN, MSN, CPNP‑PC, CCRN
Advanced practice clinicians treating patients in a variety of settings and specialties
Learn more about In Practice: Reflections from NPs and PAs.