
July 10th, 2015
Transitions of Care
Andrew Ip, MD

Andrew Ip, MD, is a 2015-16 Chief Resident in Internal Medicine at Emory University in Atlanta, Georgia.
Brief HPI: 3rd year resident, Asian-American male, from Philly, presented to Emory University as a wide-eyed intern July 2012, currently admitted to become a new Chief resident at the VA
Meds: see EMR
Pertinent Labs: see EMR
Top Active Problems:
- Computer Codes – missing but awaiting IT approval
- Awaiting MRI of brain past 48 hrs – syncope work up
- Psychosocial – extremely anxious to start chief-ing and leave behind a transformative experience in residency
Sign-out: NTD overnight
Anticipatory Guidance: If starts to have a panic attack about being chief, ok to give Haldol 2 mg IM
Medical transitions of care are never easy – just the thought of signing out patients to a night float resident frightened me as an intern. Even as an upper-level resident, I was unsure at times of my ability to properly hand off patient care. The above example follows a standardized format to give a cross-cover provider a succinct overview of a patient’s care, but things do get lost in translation. There is no better example of this at my residency program then the ICU month at our public safety-net hospital, Grady. Below is a graphic of our ICU sign-out structure:
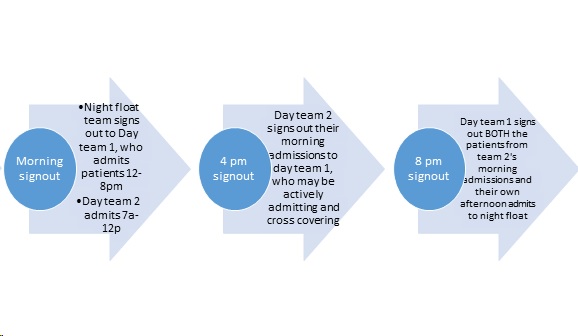
Our ICU signout process
This format keeps a team (1 resident, 2 interns) intact by avoiding any 24 hour calls; however it was extremely prone to sign-out mishaps and fragmented patient care. One case I will never forget ended up with a patient coding, likely due to hypoglycemia. During verbal sign-out rounds at 8pm, no one mentioned hypoglycemia; in fact, the call team (day team 1 in above graphic) did not even know much about the patient’s history or reason for ICU admission. The written sign-out also left out the critical information that patient had a blood glucose of ~25 on arrival to the ER. This was the infamous sign-out of a sign-out we all dread from multiple departments, let alone in the MICU.
While medicine transitions of care sometimes leaves a sour taste in my mouth (thankfully, iCompare, the flexible arm, will allow for a MICU 24-hour call system and hopefully address these sign-out issues), I want to now focus on a much different, non-medical transition – leaving residency.
As I signed out in the beginning, I’m going through the initial pangs of transitioning to my new role as a chief resident. It is a wonderful opportunity to teach, mentor, and work on the administrative side of academic medicine. But leaving behind the wonderful class of 52 residents I’ve worked with, laughed with, and cried with has made this transition so bittersweet.
Graduation June 17, 2015 for Emory Internal Medicine residents. Photo taken by Terrance Mason ™
Many in my class will move away from Atlanta, GA — in fact, will move to 13 other states by my count. The time I’ve spent the past 3 years with these individuals has been transformative, a thorough ‘through-the-fire’ refining. Residency launches many of us into a maelstrom of clinical duty mixed with scholarship and rounded out with lifelong bonds formed from shared experiences that only other co-residents can understand. My experience was so intricately tied with who I worked with that I know the friendships and memories made will endure much longer than my career. So if you’re a graduated resident, a graduating resident, or even a budding student doctor, remember to cherish the people you work with and the memories you make along the way.

At wedding of 2 Emory medicine residents!
One part of me is excited to transition to my new role as a chief resident, but the other part of me, ironically, doesn’t want to sign out of residency. Is that so wrong?
I would love to hear other people’s thoughts on transitions in their medical training, or even thoughts on transitions of care within the hospital!
5 Responses to “Transitions of Care”

2021-2022 Chief Resident Panel
Abdullah Al-abcha, MD
Mikita Arora, MD
Madiha Khan, DO
Khalid A. Shalaby, MBBCh
Brandon Temte, DO
Resident chiefs in hospital, internal, and family medicine
Learn more about Insights on Residency Training.
 NEJM Journal Watch – Recent General Medicine Articles
NEJM Journal Watch – Recent General Medicine Articles- Are Automated Insulin Delivery Devices Useful for Patients with Type 2 Diabetes?
- Does Prone Positioning Save Lives in Nonintubated Patients with COVID-19?
- Surgery vs. Nonsurgical Management for Cervical Radiculopathy
- Interventions for Intermediate-Risk Pulmonary Embolism
- Do Statins Affect Risk for Developing Hepatic Decompensation and Hepatocellular Carcinoma?
Dr Ip
Thank you for a witty and thought-provoking article. Well done!
Congratulations to you and your classmates and best wishes as you embark on your careers. 13 states — wow, that’s a prety good Hegira!
Hi,
Thanks for being so honest about it. I am going to apply this year in Emory for Int medicine residency. Hope to get an awesome experience if I get accepted.
During my nightfloat hospital experience I always felt verbal sign out format is less time consuming but probability of human error is also higher. It freaks me out sometimes.
I also enjoy teaching side of medicine as a tutor to help students with USMLE. It is the best way to comprehend medicine and keep ourselves up to date.
Thanks for sharing your experience and emphasis on cherishing moments with colleagues.
Dear Dr. Ip,
You have a sensitive nature-nurture this and be compassionate. There will be trying times, remember, the best swords are forged in high heat and pounded many times to create a finely tempered weapon. You are a weapon against human disease and suffering. Good Luck!
Carl K. Yorita, MD
Internist
Thank you for writing this. I find your sign out hilarious!
You are absolutely right that transitioning to a different medical training is so difficult, and one of the main reasons are the co-residents you have spent with for 3 years. We have created a blog and whatsapp group for people to update their life once in a while and to make sure we keep in touch!
Dr. Ip,
Fascinating and well written.
Something we are attempting at our hospital to help with transitions of care is the “Patient Acuity Rating”, a score of 0-7 given to patients’ “sickness” based on acuity. It may not be as relevant in the ICU, but a recent study at the Mayo clinic showed very good results.
Interns who rated someone at least 5 were up to 12x more likely for clinical deterioration within 24 hours. Third year residents who rated patients 4+ were up to 18x more likely to get very sick within 24 hours.
Always good to continue adjusting as we go through this time of change in residency!
Article: http://link.springer.com/article/10.1007%2Fs11606-014-3114-4