
June 16th, 2022
Dear Chief Year …
Madiha Khan, DO

Dr. Khan is an Internal Medicine Chief Resident at Houston Methodist Hospital in Texas.
If you ask anyone on Reddit or SDN (Student Doctor Network) about pursuing Chiefdom in residency, you’ll find numerous opinions about it being an undertaking not worth the burden of additional responsibilities, even if it is considered an honor. I was also advised gently — and accurately, in my opinion — by mentors that focusing on research would lend itself to a ‘stronger’ fellowship application, because chief selection is not standardized across all programs, which makes it difficult to gauge just how much of a positive it is. (Particularly when it is not the traditional extra year as a PGY-4.) Honestly, while I never thought it would help secure a fellowship spot as much as other pursuits might have, I did feel that it would invaluable for an eventual career in academics. Besides, I love emails, email templates, and the slew of operational management conundrums that most people dread, so I thought perhaps the addition of administrative responsibilities wouldn’t be that much of a time-sink for me, at least.
I was wrong.
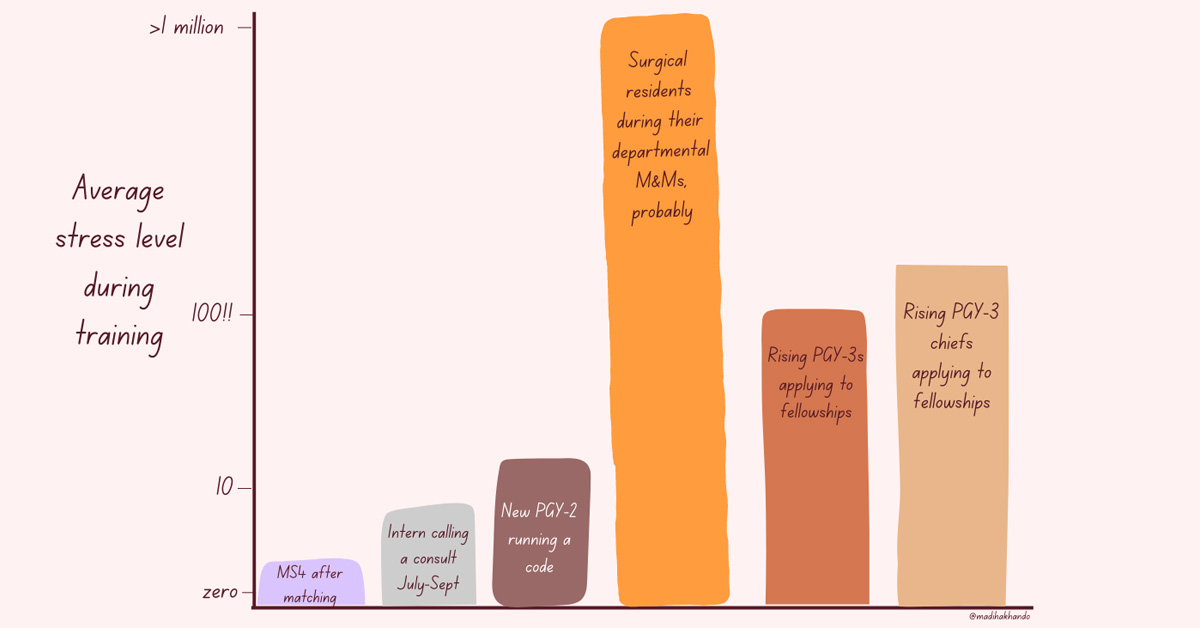
Truthfully, since the day my two co-chiefs and I were elected in March 2021, it has been a humbling, non-stop grind, with moments of self-doubt and even regret about our choice at times. For me, balancing chief duties with clinical responsibilities while also applying to fellowship made it easily one of the most stressful periods of residency (a rough scale of my individual perception of average stress levels in training is included below). However, reflecting back on this time, these struggles yielded not only great personal growth, but meaningful improvements for our program that made this grueling experience a success and truly worth it in the end… and sometimes, even fun.
At our mid-sized program, the three chief residents (typically PGY-3s) function as one unit. There are no designated roles or distinct labels for each chief (e.g., curriculum or administrative chief). Instead, we had the internal autonomy to divide all educational/administrative work amongst ourselves. For this reason, my experience of having a “successful” chief year is intertwined with the experience of my beloved co-chiefs. Although we spent the past year speaking as one voice, I want to share some insights regarding the challenges and successes of this past year, as one leg of an objectively solid tripod.
 Positive Feedback Loop
Positive Feedback Loop
Now that the year is nearing a close, we feel very fortunate to be able to look back at this journey with both pride and contentment that our conscientious leadership was mostly well received and met with tangible positive results: From implementing changes behind the scenes to changes that directly affected residents on a day to day basis.
Since ‘improvement’ can be subjective, not every change was met with enthusiasm, and the sting of rejection would unearth feelings of demotivation. However, with each win, we felt more equipped to cast our net wider and diversify areas of improvement, to a point where it felt like an avalanche of changes in a short amount of time. Win, lose or draw — we learned a lot about the process of getting good ideas approved, and subsequently, getting them practically implemented. Although we became more efficient, the workload did not seem to shrink, as more complex issues required more well-thought out solutions. But, the snowball of successful changes provided the confidence and fuel to take on more, and this was one of the key aspects that blunted burnout. The momentum of approvals energized us enough to keep asking “what else can we improve?”
No Chief Is an Island: Being Set Up for Success
Several months into the chief year, we had made a lot of changes. Internally, we had overhauled our workflow for making schedules and fairly utilizing jeopardy coverage (read: got intimate with Excel), beefed up for recruitment season by investing in the residency social media, and gave the residency website a facelift while also troubleshooting ways to make it secure enough to serve as a platform for internal learning. In the midst of recurrent whiplash of virtual versus in-person mandates, we brainstormed ways to keep the didactic and clinical curriculum robust by negotiating with other subspecialties to find a sweet spot between coverage and teaching that worked for the residents. Somewhere along the way, we also hosted a regional conference for the local IM programs, but my memory of that time is limited to this picture:

My co-chief Rafid Jahan and I hosting a tiny desk conference (aka ACP Associate’s Day 2021)
I list all this not to provide a laundry list of tasks we accomplished, but to convey that these changes would not be possible in such a hectic and dynamic environment without:
1) Motivated residents that took the time to give fair, honest, and frequent feedback during growing pains. When all parties have a vested interest in the future of the program it ensures a better experience not just for the current residents, but future ones too.
2) A Program Director and faculty willing to listen and seriously consider proposals, and advocate for residents.
3) A Program Coordinator that guided us through the basics, which gave us the opportunity to not only understand the context of the duties of chief residents, but to also reach beyond and enact practical change while respecting the ecosystem in which a program operates.
Chief residents (PGY-3) are not yet viewed as full-fledged programmatic leadership and also not quite viewed as an average resident. It is this unique perspective of access to bits of privy information that allowed for identifying gaps in the optimal resident experience (whether curricular or wellness related) and the ability to implement changes.
Long story short — this is how we lobbied for and secured a ping pong table for the resident lounge.
X+Why: The Biggest Improvement I’ll Never Experience
Mid-morning of December 1st, aka Fellowship Match Day, my co-chief Ibrahim and I breathed a sigh of relief: We had matched! Although our co-chief Rafid was spared from the second round of ERAS as a future hospitalist, he probably breathed a sigh of relief too, maybe even deeper than either of us. At this point we had been ‘chiefing’ for more than 8 months. In that time, we had made a lot of strides. We felt good about our work and felt even better that we successfully matched, despite spending so much time on things outside of the fellowship match. Then, later that day, we received a text from our PD:
Great work guys! Now onto finishing the X+Y schedule, that will be your real legacy as Chiefs.
Up until now, I had thought our legacy was the ping pong table, or maybe shortening the deadline to request PTO. During the commotion of the first half of the year, we had put implementation of a totally new and improved scheduling model on the back burner. Briefly, our program functioned with the traditional model of clinic, meaning that during inpatient months we would leave for a half day to go to our continuity clinic, and it was now time to switch to a more progressive system.
Instead of providing a walkthrough on transitioning to X+Y, as this can be program dependent, I will share the factors that helped us rally to undertake the biggest improvement yet.
Beyond the three of us genuinely sharing the unified goal of improving the program, I would say the most important aspect of undertaking such a task was the fact that we had the confidence and trust of our leadership to take the reins and be successful and were given the bandwidth to do so. Micromanaging can quickly handicap motivation. We were set up for success because we weren’t limited by micromanagement. To be clear, we did go back and forth on details, but amongst each other — so by the time we were ready to propose our suggestions, we had a good understanding of what criticisms could arise. Thus, we felt pretty confident that our proposals would be approved, as they were extensively hashed out. Of course, systemic changes need thorough consideration and approval; however, anticipating the points that would need longer review time helped us build out a timeline that contained no lag between waiting for an answer and continuing to work on the objective.
Another crucial aspect to our success was our ability to problem-solve and internally navigate disagreements (of which there were many). Once, while creating the new curriculum, I called my co-chiefs to debrief after a particularly pugnacious day. I apologized for being stubbornly against some of the suggested changes. Then, Ibrahim said something that really struck me: There is no need to apologize for disagreements. I love and value our disagreements, because the best ideas have come to the surface when we don’t agree.
(I hope this story also gives enough context to an inside joke between us about Ibrahim: Is he the Wisest Young Man or the Youngest Wise Man?)
Would I Do It Again?
Make no mistake, PGY-3 chief year is as busy and involved as you’ve heard. Between the clinical and educational responsibilities, scheduling, recruitment, and countless administrative tasks, it is a jam-packed year. For me, however, the value of what I’ve learned about the educational system, navigating inter-professional hurdles between residents, and practicing the language of diplomacy that is required to implement changes that affect a wide range of people is invaluable. So yes, I would do it again in a heartbeat — serving this wonderful group of residents, alongside my spectacular co-chiefs, has been one of the biggest honors of my life.

2021-2022 Chief Resident Panel
Abdullah Al-abcha, MD
Mikita Arora, MD
Madiha Khan, DO
Khalid A. Shalaby, MBBCh
Brandon Temte, DO
Resident chiefs in hospital, internal, and family medicine
Learn more about Insights on Residency Training.
 NEJM Journal Watch – Recent General Medicine Articles
NEJM Journal Watch – Recent General Medicine Articles- How Do “Pay-for-Performance” Incentives Affect Quality of Care?
- Observations from ID and Beyond: Two Pandemics Compared: Reflections on HIV and COVID-19
- New CDC Guidelines for HIV Nonoccupational Postexposure Prophylaxis
- Pharmacologic Management of Neuropathic Pain
- Managing Obesity in Heart Failure: New Guidance from ACC