
October 1st, 2014
Case: Testosterone Replacement Therapy and CV Risk
Seth D Bilazarian, MD, Anna Catino, MD and James Fang, MD
A 47-year-old man presents to the hospital reporting 4 days of chest pain that occurs during treadmill exercise, left-arm and jaw discomfort, and shortness of breath with diaphoresis.
His medical history is noteworthy only for orthopedic surgeries and use of testosterone replacement therapy for reportedly low testosterone syndrome. He does not smoke and drinks alcohol only occasionally. He works as a school administrator and a high school sports coach. He has no family history of coronary disease.
The patient is obese, with a weight of 285 pounds and a body-mass index of 37 kg/m2. His physical exam is otherwise unremarkable.
His electrocardiogram is normal. Troponin I levels are 0.03, 0.04, and then 0.05 ng/mL.
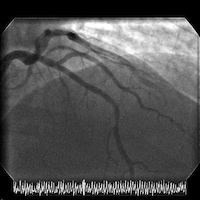
The patient is transferred to a cardiac center for catheterization in the setting of acute coronary syndrome (ACS). Cardiac catheterization reveals normal LV function and an LV end-diastolic pressure of 8 mm Hg. Coronary angiography shows a high-grade mid left anterior descending (LAD) stenosis, which is then successfully treated with a single drug-eluting stent.
Before discharge, the patient has a total-cholesterol level of 184 mg/dL, HDL of 29 mg/dL, LDL of 101 mg/dL, triglycerides of 270 mg/dL, and fasting glucose of 87 mg/dL. The patient is initiated on atorvastatin 80 mg and dual antiplatelet therapy, and he is discharged for follow-up.
Angiograms of the LAD before and after PCI with a drug-eluting stent:

Questions:
1. Did the testosterone replacement therapy play a major role, a minor but significant role (e.g., by amplifying other risk factors), or no role in this patient’s atherothrombotic process?
2. Is it safe to continue the testosterone replacement?
3. According to the ACCF/AHA risk estimator (which is not designed for use in secondary prevention), the patient’s 10-year ASCVD risk before the ACS was 5.1%; therefore statin therapy would not have been recommended. In secondary prevention, should we treat a patient who takes testosterone replacement differently than we treat a patient with multiple atherothrombotic risk factors or a higher risk according to the risk estimator?
4. When the patient’s risk is optimized, he loses weight, and he completes his dual antiplatelet therapy, could testosterone replacement be reinitiated safely (if it is stopped initially)?
5. Does the patient need lifelong statin therapy?
Response:
October 7, 2014
Questions:
1. Did the testosterone replacement therapy play a major role, a minor but significant role (e.g., by amplifying other risk factors), or no role in this patient’s atherothrombotic process?
Although observational data correlate low testosterone levels with CV risk, it remains to be seen whether treating low levels in the absence of symptomatic hypogonadism is beneficial. In fact, randomized trials of treatment for other reasons have suggested a signal of harm, particularly in patients with underlying CAD and the elderly. Therefore, a potential role for harm in this case could be made, despite the patient’s age.
2. Is it safe to continue the testosterone replacement?
We would not continue testosterone therapy without unequivocal evidence of a symptomatic hypogonadal state, particularly in light of evidence of harm in recent randomized trials of testosterone supplementation.
3. According to the ACCF/AHA risk estimator (which is not designed for use in secondary prevention), the patient’s 10-year ASCVD risk before the ACS was 5.1%; therefore statin therapy would not have been recommended. In secondary prevention, should we treat a patient who takes testosterone replacement differently than we treat a patient with multiple atherothrombotic risk factors or a higher risk according to the risk estimator?
In secondary prevention, atherosclerosis is already present, so the priority is treatment of the atherosclerosis itself to reduce the morbidity and mortality of the disease. The use of testosterone replacement should be limited to treating patients with specific hypogonadal symptoms rather than modifying atherosclerosis disease progression. Otherwise, the secondary treatment should be no different than for other patients with known atherosclerosis.
4. When the patient’s risk is optimized, he loses weight, and he completes his dual antiplatelet therapy, could testosterone replacement be reinitiated safely (if it is stopped initially)?
His testosterone levels should be re-assessed (two early morning levels, as recommended by endocrine societies) after significant weight loss. We suspect that this patient’s testosterone levels will change and may even correct if his obesity were to be reversed. Low testosterone may simply reflect other CV risk factors or be driven by atherosclerosis itself (i.e., a risk marker rather than a risk factor). If his testosterone levels remained low, we would treat only in concert with an endocrinologist if a truly symptomatic hypogonadal state could be confirmed.
5. Does the patient need lifelong statin therapy?
Yes, given that he has atherosclerosis, which needs treatment independent of his testosterone status.
Wrap-Up:
October 21, 2014
The patient was discharged the day after his successful PCI. He was seen one week later by his clinical cardiologist, who recommended therapeutic lifestyle changes, continuation of dual antiplatelet therapy, and maintenance of statin therapy (atorvastatin 80 mg, once daily). Cardiac rehabilitation was recommended, but the patient declined. The patient was advised to discontinue the testosterone replacement therapy that he had started before his myocardial infarction.
The table shows the patient’s lipid values during his hospitalization (in March) and 3 months later (in June).
|
March value |
June value |
|
| Total cholesterol (mg/dL) |
163 |
90 |
| LDL cholesterol (mg/dL) |
101 |
43 |
| HDL cholesterol (mg/dL) |
27 |
26 |
| Triglycerides (mg/dL) |
176 |
103 |
The patient’s weight fell from 285 pounds (BMI 37) to 251 pounds (BMI 34).
Despite the recommendation to discontinue testosterone replacement therapy, the patient resumed it after discussion with his primary care provider, who had originally prescribed it. The PCP recommended that it be continued, given the lack of data on potential hazards and the symptom improvement it had yielded for the patient.
8 Responses to “Case: Testosterone Replacement Therapy and CV Risk”
 NEJM Journal Watch — Recent Cardiology Articles
NEJM Journal Watch — Recent Cardiology Articles- A Less-Invasive Approach to Mitral-Valve Replacement
- Should Blood Pressure Targets Differ for Frail and Nonfrail Adults?
- Sudden Cardiac Death in the U.S.: 20-Year Trends
- Oral Semaglutide Approved to Lower Cardiovascular Risk in High-Risk Patients with Type 2 Diabetes
- Covid-19 Vaccines Improve Heart Outcomes
1. No major role as mechanistically it appears that testosterone replacement is pro-thrombotic and less so, pro-atherosclerotic.
2. No.
3. No- other than suspension of testosterone replacement therapy.
4. No
5. Probably given clinical syndrome and atheromatous burden.
For the moment We don’t know, it is very important if the testosterone replacement therapy was justify.
2. Since we don’t know the correct and safe thing to do is stop it. If he really has hypogonadism wait six month and reevaluate if is really necessary to restart the treatment.
3. No. In this case is important to evaluate the hypertrygliceridemia, the glucose is normal, measure the levels of insulin. If the glucose metabolism is normal revisit alcohol consumption and family history.
4. No, but if he really have hypogonadism you have to review the case in some cases is safe to reinitiate.
5. First by all means. But is also very important to explore insulin resistance, the presence of hypogonadism and the mechanism if really exist.
Note. The patient has not refractory Angina, hemodynamic or electrical instability, no elevated risk for clinical events, no serious comorbidities. I don’t have enough information to calculate GRACE score. This is an excellent case to discuss NSTE-ACS ischemia guided vs. early / late invasive strategy.
And check thyroid function.
Good grief –what a tangle: too many variables. I’m assuming that this gentleman had a metabolic evaluation and nothing abnormal was found. I would imagine, given the other issues when his coronary artery lesion was identified, — that if his weight issue was addressed — and his likely sedentary life style modified by instituting an exercise program, dietary modification and introduction of a statin (if hyperlipidemia or elevated cRP documented),following his coronary intervention, and attention paid to other comorbidities – and that he, without supplementation, had documented testosterone deficiency — that testosterone replacement would be reasonable. It would help to know what the initial rationale was for testosterone replacement.
Complicated stuff — but, for many, life without the ability to have sexual relations with one’s significant other may not be worth living.
1. Probably some effect. Can’t quantitate how much.
2. I wouldn’t.
3. No. Any CAD pt should have OMT.
4. I would advise him to stay off it.
5. Absolutely.
With diet, exercise and significant wt loss he might find his sexual. Inadequacy to be markedly improved without testosterone assuming he doesn’t have true hypogonadism.
NO. My MCV shot to 53 and Hct to 54—MI!! The cells, in retrospect simply could not move well through the LAD stenotic area. Now stented on indefinite prasugrel therapy. It was not fun. Shot my practice, energy and life to hell. Values seen in retrospect ESP in highly calcified area. (Ebct). Even more to the story when a VA gp stopped the initial plavix, would not call my cardio or call upstairs to theirs for a second opinion. Life has never been the same. Initial test. Level, repeated, was “2!” Calcium, stenosis and testosterone–set up for a disaster. dr Larry
I think this case illustrates a clear deficiency in risk calculators such as the ACCF/AHA estimators. By placing quite a bit of weight on risk associated with age and not including patient specific factors such as family history or granular measures of individual risk, I suspect they would not come in handy for a patient such as this one.
It is not as if atherosclerosis begins when you hit a certain age. With statins have low risk, why not begin one sooner in this gentleman.
I would argue that an almost morbidly obese patient in clinic with clear signs of metabolic syndrome likely needs a combination of lifestyle and medical therapies to ward of a cardiac event. I would not be surprised if he had an MI without being on testosterone, and it would be hard to quantify its contribution to this event. That said, I would not continue him on testosterone unless an endocrinologist strongly felt that he needed the replacement (i.e. this was not a soft diagnosis of “low T”).
He has bought himself lifelong statin therapy as well as cardiac rehab.
I am surprised that his LVEDP during an ACS was only 8mmHg.
Tariq is correct, the traditional risk calculators are terrible. Too bad this subject did not have a coronary calcium score performed which would have diagnosed his high risk and resulted in initiation of therapies prior to his event. Perhaps this event could have been prevented.