
May 5th, 2017
Deep Brain Stimulation Targeting in Neurosurgery, Part III of III
Bianca Belcher, MPH, PA-C

Bianca Belcher, MPH, PA-C, practices neurosurgery in Boston, MA.
This is the final part of a three-part series on deep brain stimulation (DBS) targeting designed for providers who lack an intimate level of knowledge and/or experience with this subject matter. In Part I, I discussed the ventralis intermedius (Vim) target as well as an overview of DBS, equipment, and programming, and Part II covered the globus pallidus internus (GPi). This final part is a review of the subthalamic nucleus (STN), the default target in some institutions. There is more scientific literature about the STN than about other targets [1], but this is changing.
Subthalamic Nucleus (STN)
Where is it located?
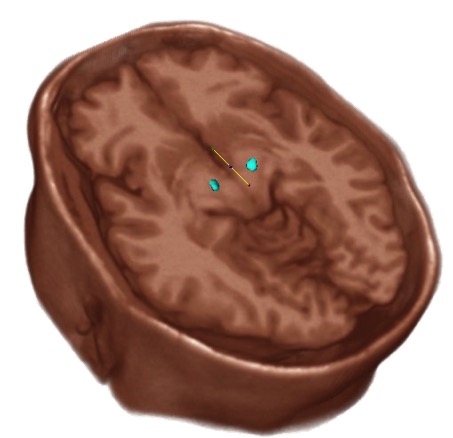
The STN is located just below the thalamus at the posterior limb of the internal capsule, medial to cranial nerve III, and inferior to the substantia nigra.
 Indication for Targeting:
Indication for Targeting:
- Parkinson’s Disease (PD)
- Stimulation of the STN treats the cardinal motor symptoms of PD more effectively than GPi or Vim.
- Patients with severe “ON/OFF” fluctuations tend to do better with STN lead placement.
- STN placement provides the best chance of achieving post surgical medication reduction.
- The STN, a smaller target than the GPi, often requires lower voltage to achieve symptom relief, leading to less frequent battery changes. If a patient is young and may require several battery changes over their lifetime, this may be a secondary consideration after optimal symptom relief. Of note, there is a rechargeable battery on the market that may negate this consideration in some patients.
Cautions:
- If dystonia is present, stronger consideration is usually given to GPi placement over STN.
- Psychiatric comorbidities in patients can be exacerbated with stimulation around the STN. Our patients undergo neuropsychological testing prior to target selection to mitigate this risk.
Adverse side effects of stimulation based on location of electrode in relation to optimal placement [2]:
Too lateral – With stimulation of the motor and frontal eye fibers of the internal capsule, the patient would experience muscle contractions, dysarthria, and contralateral gaze deviation.
Too medial – Diplopia, eye deviation, sweating, nausea, depression, and personality changes can all be a consequence of stimulating medial structures such as the nerve roots of CNIII, the red nucleus, or the ventromedial portion of the STN.
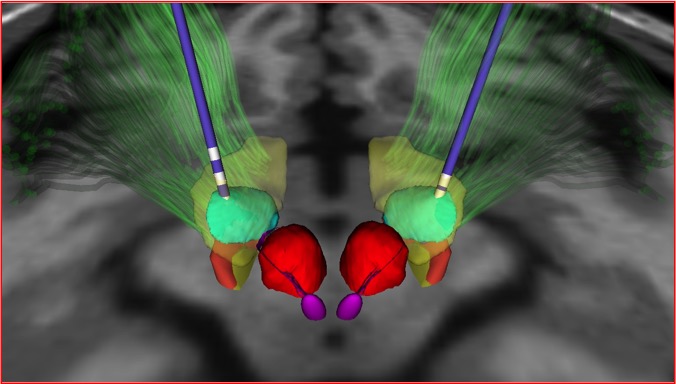
Green, STN. Red, Red nucleus. Purple, Oculomotor nucleus of CNIII. Blue, medial lemniscal pathway.
Too posterior – With stimulation of the medial lemniscus, the patient will experience paresthesias.
Too anterior – The patient will experience muscle contractions and autonomic symptoms such as panicky feelings or sweating due to stimulation of the hypothalamus or motor fibers of the internal capsule.
Too superior – No effect on tremor
Too deep – Mood changes and muscle contractions due to stimulation of the substantia nigra or the internal capsule
References
- Deep Brain Stimulation Management. William J. Marks, Jr. Cambridge University Press 2010
- DBS Anatomy & Side Effects. A Presentation by Kirk Finnis, PhD. Medtronic.

One Response to “Deep Brain Stimulation Targeting in Neurosurgery, Part III of III”

NP/PA Bloggers
Elizabeth Donahue, RN, MSN, NP‑C
Alexandra Godfrey, BSc PT, MS PA‑C
Emily F. Moore, RN, MSN, CPNP‑PC, CCRN
Advanced practice clinicians treating patients in a variety of settings and specialties
Learn more about In Practice: Reflections from NPs and PAs.
That is really a very good explanation of DBS in Neurosurgery!! Thanks, Bianca!!