
An ongoing dialogue on HIV/AIDS, infectious diseases,
December 12th, 2015
The 2015 ID Fellowship Match “Historic Bad”: Part 1, Debating the Cause
This year’s ID fellowship match has just taken place, and the results were, ahem, not pretty. Part 1 will cover why we’re in this situation; in Part 2, I’ll offer some reasons for optimism, and even some solutions.
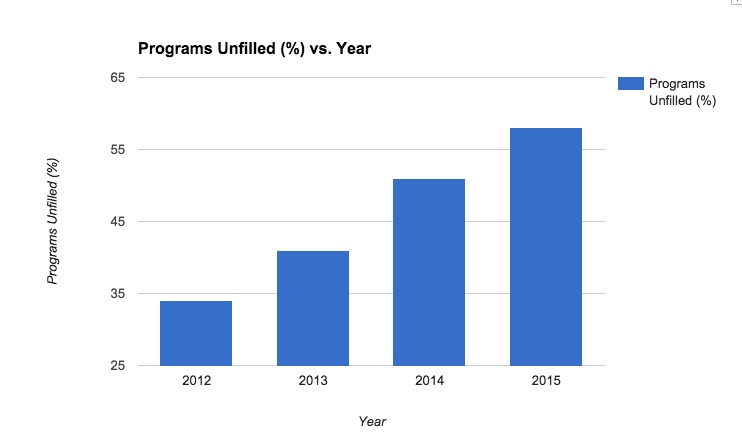
According to data provided by NRMP, 117 of the 335 ID fellowship positions were unfilled. Dan Diekema from U of Iowa, who has written frequently on the issue of the ID match, quickly calculated that over 80% 80 programs had at least one unfilled spot.
[That was an important edit — please see Dan’s comments below.]
When I cited this alarming figure, it generated a spirited email exchange about the ID match with Emory’s Wendy Armstrong, the source of the “historic bad” quote in the title. Wendy is also IDSA Chair of the Task Force for Recruitment to ID, so has thought a lot about this issue.
She acknowledged the trend is worrisome:
The bulk of our exchange, however, was about the reasons for this alarming trend.
Her view: It’s multifactorial: Limited ID teaching in medical school, with declining numbers of dedicated microbiology/ID courses. A significant proportion of preclinical curricula are led by microbiologists alone. ID faculty have less exposure to medical students in the hospital. There are fewer clinical electives for residents. There are fewer ID clinicians acting as attendings on medical services. It’s the money.
My view: It’s the money. At least, it’s mostly the money.
Yes, the factors listed by Wendy are part of it. But since several apply to other medical subspecialties — how many cardiologists or gastroenterologists attend on general medical services? — I’m not sure they are playing much of a role.
Why is the money issue important, and why is it particularly bad for ID? A few thoughts:
- Debt. Undergraduate medical education in this country is expensive, and a substantial number of doctors in training have significant medical school debt. They look at the 2-3 years of extra training required to become an ID specialist — followed by a lower salary — and cross ID off their list. Or at the very least, strongly consider other options if they are undecided. Or, as put succinctly here:

- The volume/procedure deficit. So long as clinicians are reimbursed primarily based on volume and procedures, ID specialists will be at a disadvantage. Medical complexity and our drive to get the details just right limit the volume part of the equation — you just can’t rush most ID consults, it would be like trying to write a guide to the Louvre after visiting for 30 minutes — and we are not trained to do procedures.
- The “lifestyle” issue. The revenue disadvantage from not doing procedures is shared with other cognitive specialists, of course, but few have so much of their work focused on hospitalized patients. Importantly, nephrology is the other major specialty with declining numbers of applicants, and I don’t think it’s a coincidence that nephrology also has plenty of hospital work. Hospital-based specialties require extensive weekend and evening call for urgent cases — cases you have to come in and see, not manage from home. Here’s a comment on my wife’s primary care listserv discussing the 2015 ID match:
ID doctors are always the ones at the hospital late at night working at our hospital. And not compensated for it they way they should be. Many are of retirement age. Only a few younger guys.
Could it be that potential applicants see ID doctors staying late in the hospital, coming in during the weekends and holidays, and wonder — why should I do that and get paid so (comparatively) poorly? The contrast with cardiology, gastroenterology, and intensivist doctors from a reimbursement perspective is obvious.
- Primary care subsidies. Primary care providers are also on the low end of the salary scale, but they rarely do extra years of training after residency. Furthermore, primary care practices may be subsidized, both explicitly through the ACA and as a way of large healthcare systems increasing the number of “covered lives”. Again, from the listserv:
I worked in HIV clinic in urban city in NJ and couldn’t believe what a new grad starts at…one did his fellowship at our hospital and was offered $85k in a private practice and the other was offered $110 as a assistant director so a lot of administrative, teaching, and research in addition to seeing patients. He had to moonlight in the prison system just to make his student loan payment!
Certainly here in Boston, and anecdotally elsewhere, PCPs start at a significantly higher salary than ID doctors.
- The rise in hospitalist positions. The winners in this race to a “real salary” in Internal Medicine? It’s the hospitalists, whose salaries generally exceed those of many ID doctors who have been in practice for years. It’s no wonder that many ID applicants today have spent at least a year after residency as a hospitalist, essentially extending their residency in terms of clinical activity, but now getting paid a whole lot more. How many of these hospitalists once considered ID training, but decided ultimately it wasn’t worth it? Longer hours for less pay, no thanks!
- Biology. In my highly unscientific poll of friends and colleagues, the period at the end of residency is the most common time for doctors to start thinking seriously about starting a family — or, in some cases, actually having babies. Such a major change certainly brings the debt, salary, and lifestyle issues cited above into stark focus.
Reading the above, you might think I’m pessimistic about the future of our speciality, but — call me crazy — in fact the opposite is true. Having one dominant cause to the problem is in many ways easier than a highly complex, multifactorial situation. Fix the money problem, and the interest in ID will rebound nicely.
In Part 2, I’ll try to justify my optimism.
Here’s a relevant 80s classic:
[youtube http://www.youtube.com/watch?v=pp4suZ4jNXg&w=420&h=315]
22 Responses to “The 2015 ID Fellowship Match “Historic Bad”: Part 1, Debating the Cause”

Paul E. Sax, MD
Contributing Editor
NEJM Journal Watch
Infectious Diseases
Biography | Disclosures | Summaries
Learn more about HIV and ID Observations.
 NEJM Journal Watch — Recent Infectious Disease Articles
NEJM Journal Watch — Recent Infectious Disease Articles- Innovative Pairing of Beta-Lactamase Inhibitors to Combat Multidrug-Resistant Gram-Negative Pathogens
- Ceftobiprole Joins the Beta-Lactam Squad Against MRSA Infections
- Sulbactam-Durlobactam for Treating Patients with Acinetobacter baumannii Infections: Do MICs Matter?
- Antibiotic Options Against Enterobacterales That Produce Wild-Type AmpC β-Lactamases
- Quorum Sensing in Pseudomonas aeruginosa — An Overlooked Treatment Target?
Hi Paul,
Thanks for your post linking to our blog, but I must correct your statement above. If you go to my post you’ll see that I never said more than 80% of programs were unfilled. My graph is clearly of the number (N) unfilled, and in the text I correctly stated that over 60% were unfilled. A dumpster fire either way, but I don’t want anyone to think my math is that sloppy. Please tell Wendy that my numbers were, in fact, “quite right”.
Thanks,
Dan
…..sorry, “about 60%” was my statement.
Dear Mike,
My apologies for the mis-read. I’ll correct the post.
The message is the same, as you note!
Paul
Is there access to the NRMP match results by program released to the general public so that residents, like myself, who are interested in ID 2016-2017 appointment would be able to target unfilled programs (my wife is pending OB-GYN residency match so no decisions till March can happen on my part but it can alter our rank list)?
Thanks, Paul,
It’s actually Dan, but thanks for correcting the % to a number. However, the post still reads as if I exaggerated the problem (“Dan’s figures aren’t quite right…the numbers…are not that high”). My match day post reported the numbers accurately, the exact numbers NRMP reported immediately after the match: 82 unfilled programs, 117 unfilled positions.
Sounds nitpicky I realize, but our blog has had a back-and-forth with IDSA leadership about this issue, and the last thing I want is for them to think that we are intentionally exaggerating the problem.
Best,
Dan
Dan, amplified the edit, and removed mention of our mis-read of your post. But it’s clear we all acknowledge the concerning trend. And for the record, speaking as an IDSA member, I do not think you are exaggerating one bit!
Apologies again.
Paul
Dear Tim,
I believe that your IM program director should be able to get an updated list of unfilled programs and spots that includes contact information for the ID PD at each site (unfilled programs have been slowly filling post-match, and when they do fill a spot they inform NRMP). I think you will find several options, but now is definitely the time to contact programs!
Your situation brings up a related concern for the ID Match….residents now know that spots in excellent programs are open after the match, which reduces the urgency to enter the match and spend valuable time and money interviewing (not to mention the stress of multiple long interview days). So some may be sitting out the match and then making their decisions afterwards. This makes it even harder to get a handle on the true extent of the mismatch between supply and demand, though I think the IDSA tracks the total number of matched applicants and when they matched (pre-match, match, and post-match).
If you have trouble finding what you’re looking for, email me at dan.diekema@gmail.com and I will send you the match day list.
Best,
Dan
With tuition and med student debt rising, and with ID now being the lowest paid specialty in medicine, who will deal with the next global influenza pandemic? Who will address the growing epidemic of antibiotic resistance? Who will put be left to don the space-suits and risk their lives taking care of people with Ebola…or with whatever disease comes after it? To be an infectious disease specialist you first have to be an internist. Does it make sense that your salary should DECLINE if you decide to do 2-3 years of additional specialty training in a field that is desperately needed. Unfortunately, the ACA didn’t address this issue as it should have. We continue to reward doctors for doing things TO people, but not for taking care OF people…and in this case, of the health of the world.
My $20,000 debt was paid off during fellowship. Salary, and the need to pay off mortgage-sized loans, never entered my mind when choosing a specialty.
Tim–You can also look on AAMC’s “Find A Resident” site where there are programs advertising openings. There are currently advertisements for 8 ID positions on the site (including our program–“shameless plug”).
Best of luck to you,
Beth Gadkowski
Eastern Virginia Medical School in Beautiful Norfolk VA
Why is anyone surprised the ID match is so poor?
The majority of graduating medical students face a mountain of debt to repay. Clearly these individuals are choosing careers where their income will be maximized and, let’s face it, ID has the poorest income flow of all.
Dr. Sax –
Agree with all of the points as above! It seems clear to me that we should advocate for a small share of some of the bundled payments that other services receive. For example, we take donor transplant calls and advise yay/nay to the surgeons re: whether or not to transplant based on donor infectious risks. 3, 6, 12 month, 5 year transplant outcomes are fundamentally affected by this often nuanced and complicated (and often middle of the night) judgement but we get no reimbursement for this!! We cannot continue to recruit the best and brightest if we are giving away our services for free, bearing the aforementioned burden of the expectation that we will be available at a moment’s notice anytime of the day or night, and shouldering the responsibility of these difficult decisions with none of the remuneration!
-Kate Mullin
I really appreciate the thoughtful comments and feel the pain of the ID community as it struggles w/unfilled slots. I’m a clinical educator (not ID trained), though I have a tremendous amount of respect for the field and highly value the input of my ID colleagues. A few thoughts about the drivers:
1. My school (University of California, San Diego) has a pretty robust ID themed block in the first (pre-clinical) year, which is organized by very smart and capable clinical ID faculty. This includes lecture, small group, and PBL work. So, our students are exposed early-on to ID in a good light – yet I don’t think this has much impact in terms of later training choices.
2. Clinical ID consult work is based on classic dig-thru-the-data, careful review of all the details, thoughtful hx/pe and conversation w/all involved parties. This is clearly labor intensive, yet is the cornerstone of good care. That said, I don’t think it’s viewed as appealing or as acutely rewarding as some of the other clinical fields where direct interventions yield immediate results. In addition, as mentioned, the $/hour are low.
3. I know that the ID community is well aware that the Antibiotic choices typically made in the clinic and hospital aren’t necessarily done with optimal care and attention. With resultant well described negative downstream consequences (i.e. increased cost, c dif, resistance, etc). I mention this because perhaps aggressive antibiotic stewardship could draw attention and support to the ID world. If hospitals recognized that cost and length of stay could be decreased by more active abx management, then this could (maybe) bring more $s to ID services/clinicians, who are best positioned to provide these services.
Hang in there.. and thanks for the Cyndi Lauper video..
Charlie Goldberg, md
Many of the preceding comments center on the role of salaries in the declining interest in ID as a subspecialty. At the root of this is the often mentioned fact that procedures are reimbursed to a much higher level than “cognitive” care. I would really appreciate a discussion of why this is the case. How did this system of bias in reimbursements evolve? Who/what is responsible for maintaining it? If the root cause of declining interest in ID as a subspecialty is truly low salaries, then addressing this problem will require addressing disparities in reimbursements.
Al Hauser
Please don’t take too long to post Part 2 and offer some optimism.
Dear Paul,
Thank you for this blog. I am a microbiology (CM) resident in Belgium, Europe and we are facing comparable problem. It is also quite difficult to find medical student who want to specialize in microbiology (CM) and in ID.
I might add an additional reason for this: our own succes. Due to succesful infection control program, we have less to do with infectious disease. Also, students do not encounter diseases as they read in text books and it might keep them away from CM/ ID.
About money, I have mixed feeling. In the low lands in Europe (Belgium, The Netherlands), CM is one of the well paid specialties. But the job prospective is not so good. Hospitals do not need many CM/ID specialists due to relative low number of infectious cases.
Erlangga Yusuf, MD, PhD
Unfortunately, ID seems to be the only specialty where we need to show our value.
The closest specialty to ours may be Heme-Onc (in term of being -mostly- a cognitive specialty); no non-oncologist would imagine starting a patient on R-CHOP, but basically anything goes with almost any antibiotic/antiviral, despite proving again and again that this leads to many poor outcomes (ok, most chemo regimens are much more toxic than antibiotics, but antibiotics are many-folds more abused/overused/misused).
Thank you to Dr. Sax and to all the other thoughtful contributors.
I finished my ID fellowship 40 years ago. I love this specialty. In my experience those who have chosen this specialty tend to be the best and most thoughtful of physicians. Concerns about reimbursement disparities did not much cross the minds of most ID fellows back then (1970’s). What a different world it is now. By the time I decided to limit my practice one of the principal reasons was that I could no longer pay my overhead and make even a modest income.
So even for me it turned out to be “all about the money.”
And many thanks for the link to the Cyndi Lauper music video. It left me really smiling.
I agree with the primary driver being salary and comments by others above–I would add that I think job security is also seen as an issue by prospective ID fellows:
1. There is a perception (I think probably true?) that ID jobs outside of an academic setting are hard to come by and are likely to be at least partly primary care, partly ID. So why do extra years of training ID fellowship when most of your work is going to be PC anyway (particularly as a lot of potential overlap in the type of people who want to do primary care and the type of people who want to do clinical ID)
2. There is a perception (I think probably true) that the NIH research pathway via K award is becoming harder, or at least taking longer. This means less perceived chance of success at a research career if there isn’t a very strong background going into fellowship– or a prolongation of fellowship (longer period of lower salary) and a need to negotiate divisional support during a donut hole of funding in a specialty where clinical work is not extremely lucrative (and therefore not easy to just ‘do more clinical time’ while awaiting a research development award).
ID interested residents that I have talked to have indicated that these issues, in addition to the lower salary overall, push them more towards being hospitalists, PCPs, doing liver/GI or critical care specialties.
I think more than absolute numbers (because by most standards we are well paid), it is perhaps the disparity between our salaries and those of our colleagues with whom we trained that is bothersome. As the years pass, it can be frustrating to see our co-interns who chose other medical sub-specialties ascend into higher earning brackets than ours… Primates everywhere dislike feeling like rewards are “unfair:”
http://www.npr.org/sections/13.7/2014/02/27/283348422/that-s-unfair-you-say-this-monkey-can-relate
This is about supply but what about demand? Are there quality ID jobs available with fair compensation? Hospitalist jobs are much more bountiful and diverse. It must be infinitely easier to get a Hospitalist job at a prestigious and/or urban medical center than an ID job.
I think there is another issue. I do not follow the match anymore, but I know that not long ago the fellowship application changed from 2nd year to 3rd year. I don’t have the numbers or statistics to back it up but it has been my impression that a big proportion of ID applicants are foreign medical graduates (FMG, myself included). One of the reasons is that developing countries have a lot of ID issues related to poverty/social problems, and the always fascinating tropical illnesses. Also FMG don’t carry big loans from med school, so a very high paying job is not a top priority. Most FMG come with a J1 VISA. Therefore changing the fellowship application to the 3rd year leaves only a few months to figure out what to do if you don’t match (have to leave country if nothing found, and VISA applications take a long time). So many residents may just choose to do a J1waiver job in IM instead of applying to fellowship. This will obviously affect all specialties, but since a big part of ID applicants used to be FMG, that specialty gets affected the most. Just a theory.
Hey everyone,
I guess it maybe a little late to join the discussion, however I am an applicant in the 2016-2017 season. I am applying for infectious diseases as a fellowship and am pretty certain about that. However, I eventually intend to pursue the CCM pathway w/wo stewardship. I reviewed the recently published article by Kadri et all – CCM and ID: an emerging combined subspecialty.
Is there anyway to know which programs would be accepting such applications in advance, prior to the application season? It would really help in the application process for us budding infection specialists!
Any and all help will be significantly appreciated!